
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Anatomy and Physiology of the Stomach
|Anatomy of the Ear |AP of the Oesophagus |AP of the Diaphragm |AP of the Large Bowel (Colon, Rectum, Anal Canal) |AP of Small Bowel |AP of the Biliary system |AP of the Bone Marrow |Anatomy of the Eye |AP of the Pharynx |AP of the Larynx |Anatomy of the Ear |AP of the Nose |AP of Male Genitalia |AP of the Breast |AP of the Stomach |Anatomy of the Rectum |Anatomy of the SpleenThe stomach is a muscular, J-shaped foregut organ that acts as a reservoir, a mechanical grinder, and a chemical reactor. It initiates protein digestion, sterilises ingested material with acid, regulates delivery of chyme into the duodenum, and secretes intrinsic factor for vitamin B12 absorption. Clinically, it is central to peptic ulcer disease, gastritis, upper GI bleeding, and gastric malignancy.
1) Gross Anatomy of the Stomach
- Location & relations: Upper abdomen (epigastrium and left hypochondrium), intraperitoneal. Anterior relations include left lobe of liver and anterior abdominal wall; posterior relations form the “stomach bed” (pancreas, spleen, left kidney/adrenal, diaphragm).
- Regions:
- Cardia: entry region at gastro-oesophageal junction (GOJ); close to lower oesophageal sphincter mechanism.
- Fundus: dome beneath left diaphragm; often contains gas bubble on imaging.
- Body (corpus): main reservoir and major site of acid secretion (especially along greater curvature and posterior wall regions).
- Antrum: muscular “mill” that triturates solids and mixes with gastric secretions; important gastrin physiology.
- Pylorus: pyloric canal + pyloric sphincter controlling gastric emptying into duodenum.
- Curvatures & omental attachments:
- Lesser curvature: attachment of lesser omentum (hepatogastric ligament); runs from cardia to pylorus.
- Greater curvature: attachment of greater omentum; connects to spleen via gastrosplenic ligament and to colon via gastrocolic ligament.
- Surface landmarks: The incisura angularis on lesser curvature marks the transition between body and antrum.
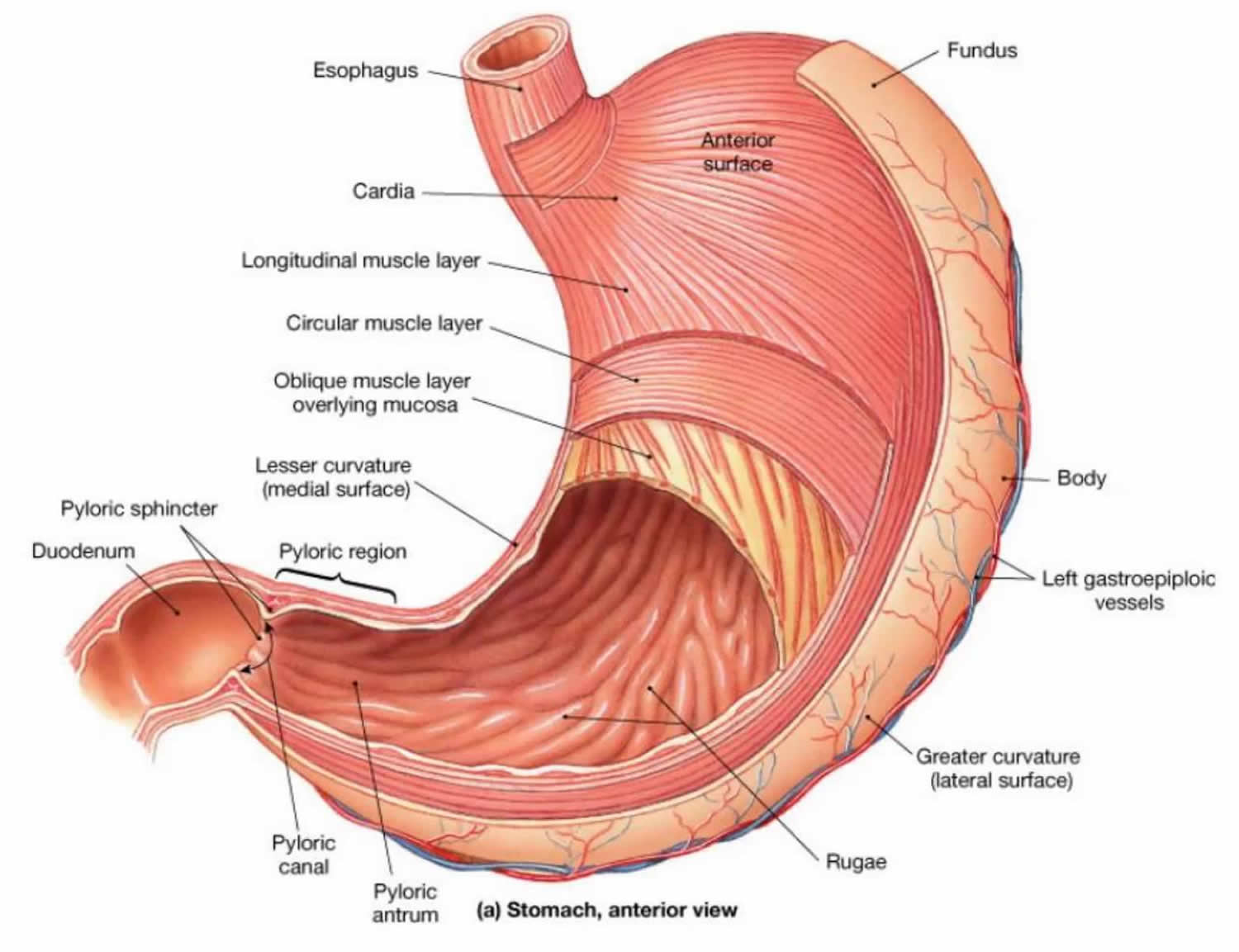
2) Layers of the Stomach Wall
The stomach wall is engineered for both secretion and powerful mixing. Compared with most of the gut, the stomach has an extra muscle layer (oblique) to enhance mechanical digestion.
- Mucosa: thick with rugae (folds). Contains gastric pits and glands; produces acid, enzymes, mucus, and hormones.
- Submucosa: connective tissue, vessels, lymphatics, and submucosal (Meissner) plexus.
- Muscularis externa: three layers:
- Inner oblique (unique to stomach)
- Middle circular (thickened at pylorus → pyloric sphincter)
- Outer longitudinal
- Serosa: visceral peritoneum.
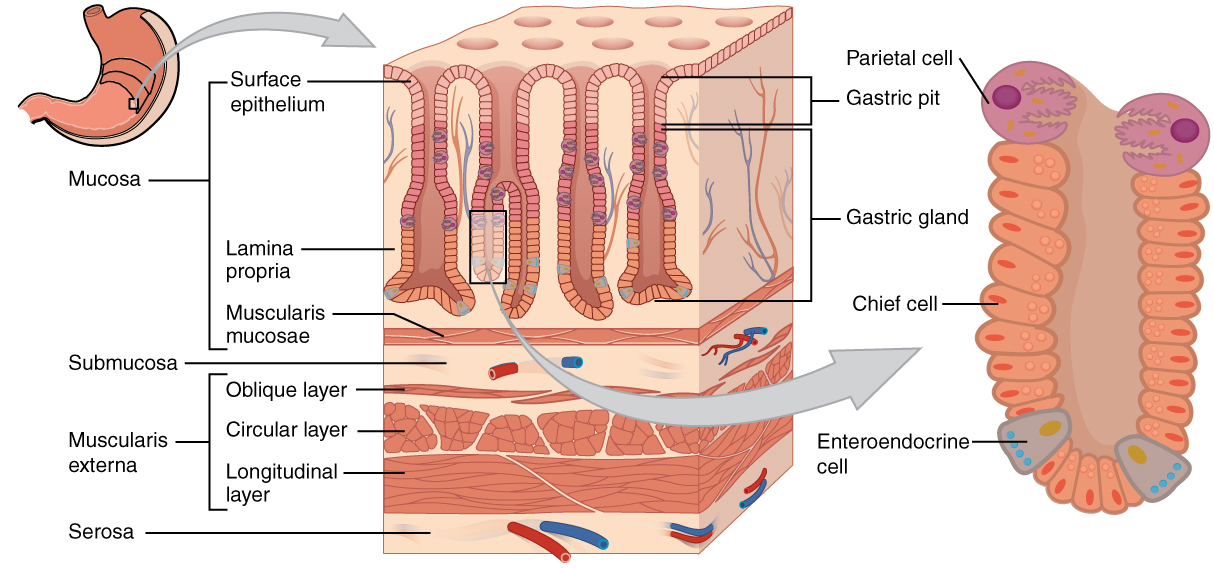
3) Gastric Microanatomy: Cells and What They Secrete
Different regions contain different gland populations. The body/fundus are acid- and enzyme-rich (parietal and chief cells), while the antrum is hormone-dominant (G and D cells).
- Surface mucous cells: mucus + bicarbonate → mucosal barrier.
- Parietal (oxyntic) cells:
- secrete HCl (acid) and intrinsic factor (B12 binding protein).
- predominant in body/fundus glands.
- Chief (zymogenic) cells: secrete pepsinogen and gastric lipase.
- ECL cells: release histamine (paracrine stimulus to parietal cells).
- G cells (antrum): release gastrin (endocrine stimulus).
- D cells (antrum/body): release somatostatin (major brake on acid secretion).
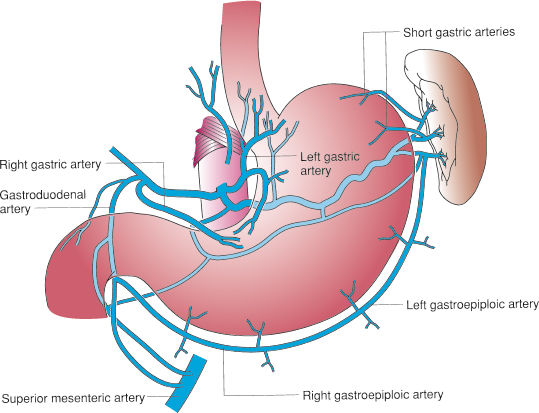
4) Blood Supply, Venous Drainage, and Lymphatics
- Arterial supply (from the coeliac trunk):
- Left gastric + right gastric → along lesser curvature.
- Left gastro-omental (gastroepiploic) + right gastro-omental → along greater curvature.
- Short gastric arteries (from splenic artery) → fundus.
- Venous drainage: parallels arteries → portal system (left/right gastric veins; gastro-omental veins; short gastrics → splenic vein).
- Lymphatics: drain along curvatures to gastric and gastro-omental nodes → coeliac nodes (important for gastric cancer spread patterns).
5) Innervation
- Parasympathetic: vagus nerve → increases secretion and motility (via enteric nervous system).
- Sympathetic: thoracic splanchnics via coeliac plexus → reduces motility/secretions; vasoconstriction; conveys pain.
- Enteric nervous system: myenteric (Auerbach) for motility; submucosal (Meissner) for secretion/blood flow.
6) Core Physiology of the Stomach
🍽️ A) Reservoir Function and Gastric Motility
The stomach must accommodate a meal without large pressure rises (receptive relaxation), then grind solids into particles small enough to pass the pylorus. This is coordinated by pacemaker activity, antral peristalsis, and pyloric “sieving”.
- Receptive relaxation: proximal stomach (fundus/body) relaxes to store food with minimal pressure rise (vagal-mediated).
- Antral pumping: distal stomach generates strong peristaltic waves that triturate solids.
- Retropulsion: pylorus closes as antral wave arrives → contents driven back for further mixing (key for mechanical digestion).
- Gastric emptying: liquids empty faster than solids; fat and hyperosmolar chyme slow emptying via duodenal feedback (CCK/secretin, neural reflexes).
🧪 B) Gastric Secretion: What the Stomach Produces
- Hydrochloric acid (HCl): denatures proteins, activates pepsin, enhances iron absorption (Fe3+→Fe2+), and kills pathogens.
- Pepsinogen → pepsin: initiates protein digestion (optimal at low pH).
- Mucus + bicarbonate: protective barrier against acid and pepsin.
- Intrinsic factor: binds vitamin B12 → required for absorption in terminal ileum.
- Hormones/paracrines: gastrin, histamine, somatostatin coordinate secretion and mucosal growth.
🧷 C) The Gastric Mucosal Barrier (Why the Stomach Doesn’t Digest Itself)
Mucosal defence depends on three linked systems: a mucus–bicarbonate layer, intact epithelial tight junctions with rapid restitution, and adequate mucosal blood flow. Prostaglandins are crucial-this explains NSAID-associated ulcers.
- Mucus–bicarbonate layer: maintains near-neutral pH at epithelial surface despite acidic lumen.
- Epithelial integrity: tight junctions prevent hydrogen back-diffusion; rapid repair after injury.
- Microcirculation: removes acid that penetrates and delivers nutrients/oxygen for repair.
- Prostaglandins (e.g., PGE₂): increase mucus/bicarbonate and blood flow; reduce acid secretion.
7) Acid Secretion in Detail (High Yield)
🔧 A) Mechanism of Parietal Cell Acid Secretion
Parietal cells generate H+ from carbonic acid. The H⁺/K⁺-ATPase (“proton pump”) secretes H+ into the lumen in exchange for K+. Chloride follows into the lumen to form HCl, while bicarbonate exits basolaterally causing the post-meal alkaline tide.
- CO₂ + H₂O → H₂CO₃ (via carbonic anhydrase) → H⁺ + HCO₃⁻
- Apical membrane: H⁺/K⁺-ATPase pumps H⁺ into canaliculi; K⁺ recycled.
- Cl⁻ enters lumen via channels → combines with H⁺ → HCl.
- Basolateral membrane: HCO₃⁻ exchanged for Cl⁻ → transient rise in blood bicarbonate (“alkaline tide”).
🎛️ B) Regulation: The “3 Stimulants + 1 Brake” Model
- Acetylcholine (ACh): vagal stimulation → M3 receptors on parietal cells and ECL cells.
- Gastrin: from G cells (antrum) → CCK-B receptors; stimulates parietal cells and ECL histamine release.
- Histamine: from ECL cells → H2 receptors on parietal cells (potent amplifier via cAMP).
- Somatostatin: from D cells → inhibits gastrin and histamine, and directly inhibits parietal cells.
🍴 C) Phases of Acid Secretion
- Cephalic phase (~30%): sight/smell/taste/thought → vagal stimulation.
- Gastric phase (~60%): food in stomach → distension (reflex) + peptides/amino acids → gastrin release.
- Intestinal phase (~10%): brief stimulation then mainly inhibition via duodenal feedback (secretin, CCK, neural reflexes).
8) Key Gastric Disorders (Clinical Correlation)
- Gastritis: inflammation (H. pylori, NSAIDs, alcohol, bile reflux); can cause dyspepsia or bleeding.
- Peptic ulcer disease: mucosal breakdown from increased acid/pepsin or reduced defence (H. pylori, NSAIDs).
📌 Complications: bleeding, perforation, gastric outlet obstruction. - GORD/GERD: reflux of gastric contents into oesophagus due to LES failure; can lead to oesophagitis/Barrett’s.
- Pernicious anaemia / B12 deficiency: autoimmune gastritis affecting parietal cells → low intrinsic factor → B12 malabsorption.
- Zollinger–Ellison syndrome: gastrinoma → hypergastrinaemia → severe acid hypersecretion and recurrent ulcers.
- Gastric cancer: risk factors include chronic H. pylori gastritis, smoking, certain dietary exposures, and chronic atrophic gastritis.
9) Diagnosis and Treatment (Overview)
- Diagnostics:
- Upper GI endoscopy (OGD): visualisation + biopsies (gold standard for ulcers, cancer, gastritis).
- H. pylori testing: urea breath test / stool antigen / biopsy urease test (context-dependent).
- FBC, U&E, LFTs: assess anaemia, dehydration, bleeding; plus targeted tests (B12, gastrin) when indicated.
- pH monitoring: for refractory reflux symptoms or pre-surgical evaluation.
- Treatments:
- PPIs: inhibit H⁺/K⁺-ATPase (most potent acid suppression).
- H2 blockers: reduce histamine-driven acid secretion.
- H. pylori eradication: combination therapy with PPI + antibiotics (per local guidance).
- Mucosal protection: avoid NSAIDs where possible; consider gastroprotection when needed.
- Surgery: for complications (perforation/obstruction) or malignancy (gastrectomy pathways).
✅ Final Summary
The stomach is a reservoir and mixer (fundus/body storage; antral grinding with retropulsion) and a secretory organ (acid, enzymes, mucus, intrinsic factor). Acid secretion is driven by ACh, gastrin, and histamine and restrained by somatostatin and prostaglandin-mediated mucosal defence-explaining the pathophysiology of ulcers and the mechanism of PPIs/H2 blockers. Its coeliac-trunk blood supply and lymphatic drainage along the curvatures are clinically important in bleeding, surgery, and cancer staging.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery