
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
The Aorta
Related Subjects: |Aorta |Acute Coronary Syndrome (ACS) General |Aortic Dissection |Acute Heart Failure and Pulmonary Oedema |Aortic Regurgitation (Incompetence) |Aortic Stenosis |Aortic Sclerosis |Transcatheter aortic valve implantation (TAVI)
🫀 The aorta is the body’s largest elastic artery, carrying oxygenated blood from the left ventricle to the systemic circulation. It functions as a pressure reservoir (Windkessel effect): elastic recoil during diastole sustains forward flow and protects microcirculation from extreme pulsatility. Anatomically, it is best understood as aortic root → ascending aorta → arch → descending thoracic aorta → abdominal aorta, each with distinct relations, branch patterns, and clinical syndromes.
🔗 Helpful links: | NHS AAA Screening (patient) | NICE NG156: AAA (diagnosis & management) | RCEMLearning: Aortic dissection classification | Radiopaedia: Abdominal aorta (radiology)
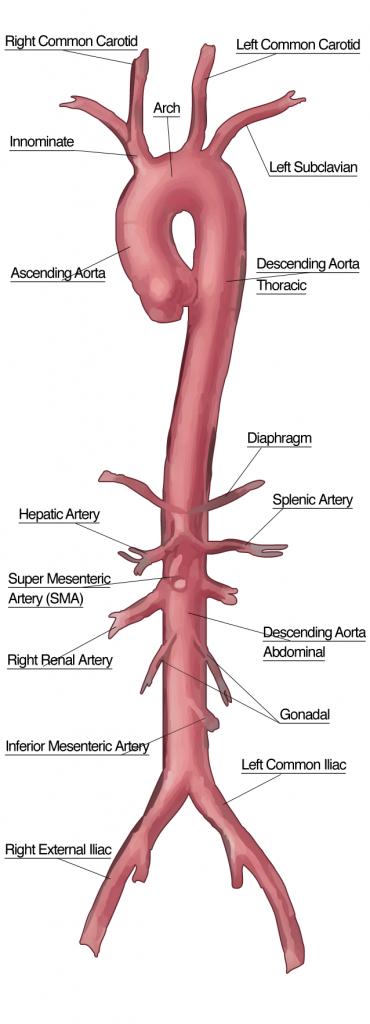
🧩 Macro-anatomy: segments, vertebral levels, and key landmarks
- Aortic root (within pericardium)
- Includes the aortic valve, aortic annulus, and sinuses of Valsalva.
- Right and left coronary ostia arise from the right and left aortic sinuses.
- Sinotubular junction marks transition from root to ascending aorta.
- Clinical: dilation of the root can cause aortic regurgitation; aneurysm here risks coronary ostial compromise.
- Ascending aorta
- Begins at the aortic valve and runs superiorly within the pericardial sac.
- Relations (high-yield): pulmonary trunk anterior/left; right atrium to the right; SVC nearby.
- Ends at the level of the sternal angle where it becomes the arch.
- Aortic arch
- Curves posteriorly and to the left over the left main bronchus (“arch over the root of the left lung”).
- Landmarks:
- Arch branches (proximal → distal): brachiocephalic trunk, left common carotid, left subclavian.
- Aortic isthmus: just distal to left subclavian; tethered by the ligamentum arteriosum (ductus arteriosus remnant).
- Relations (applied anatomy):
- Near trachea and oesophagus → large aneurysm may cause cough, dysphagia, or hoarseness.
- Left recurrent laryngeal nerve loops under the arch near ligamentum arteriosum → hoarseness can be a “mediastinal red flag”.
- Descending thoracic aorta
- Runs in the posterior mediastinum, typically left of midline, then approaches midline lower down.
- Passes through the diaphragm via the aortic hiatus (classically at T12).
- Abdominal aorta
- Begins below the diaphragm at the aortic hiatus (≈ T12) and ends at the bifurcation (≈ L4).
- Lies anterior to the vertebral bodies; the IVC is usually to the right.
- Clinical: a pulsatile epigastric mass may be felt in thin patients; expansile pulsation raises concern for AAA.
🧱 Micro-anatomy: why the aorta behaves the way it does
- Tunica intima: endothelial lining; site of atherosclerotic plaque development and intimal tears in dissection.
- Tunica media: rich in elastin and smooth muscle; provides compliance. “Cystic medial degeneration” (e.g., connective tissue disease) predisposes to aneurysm/dissection.
- Tunica adventitia: collagen-rich support; contains the vasa vasorum and autonomic nerves.
- Vasa vasorum: supply outer media/adventitia (especially thoracic aorta). Compromise can contribute to medial ischemia and weakening.
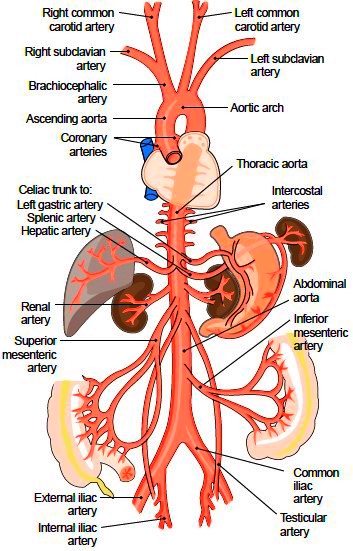
🌿 Branches of the aorta (organise by segment and by ‘visceral vs parietal’)
1) Ascending aorta
- Coronary arteries: right and left coronary arteries arise from the aortic sinuses to perfuse myocardium.
2) Aortic arch branches
- Brachiocephalic trunk → right common carotid + right subclavian.
- Left common carotid → head/neck.
- Left subclavian → left upper limb; gives vertebral artery to posterior circulation.
3) Descending thoracic aorta branches
- Posterior intercostal arteries (classically 3–11) + subcostal artery → chest wall; collateral pathways in coarctation.
- Bronchial arteries → bronchial tree (systemic, oxygenated supply).
- Oesophageal branches → oesophagus.
- Mediastinal/pericardial branches → mediastinal tissues/pericardium.
- Superior phrenic arteries → diaphragm.
4) Abdominal aorta branches (high-yield table)
| Category | Branches | Core territory (clinical angle) |
|---|---|---|
| Unpaired visceral (midline) |
🌟 Coeliac trunk
🟦 Superior mesenteric artery (SMA) 🟩 Inferior mesenteric artery (IMA) |
Foregut / Midgut / Hindgut supply (think: bowel ischaemia territories, collateral arcades) |
| Paired visceral (lateral) |
Renal arteries
Gonadal (testicular/ovarian) arteries Middle suprarenal arteries |
Kidney perfusion and renovascular HTN; gonadal pain patterns; adrenal vascular richness |
| Parietal |
Inferior phrenic arteries
Lumbar arteries Median sacral (small midline) |
Diaphragm, posterior abdominal wall; collaterals to pelvis |
| Terminal | Common iliac arteries (R/L) at L4 | Pelvis and lower limbs (internal vs external iliac territories) |
🧠 Exam memory hook: Abdominal midline unpaired branches = “CSI” (Coeliac, SMA, IMA). Pair them with renal + gonadal laterally, and finish with the L4 bifurcation.
📍 Relations and surface anatomy (why symptoms happen)
- Thoracic aorta lies close to oesophagus and left main bronchus → aneurysm may cause dysphagia, cough, or recurrent laryngeal nerve palsy (hoarseness).
- Abdominal aorta is retroperitoneal; AAA can erode vertebral bodies (back pain) or compress adjacent structures.
- Left renal vein crosses anterior to aorta under the SMA (“nutcracker” region) - helpful landmark in imaging.
- Aortic plexus (sympathetic fibres) surrounds the aorta; irritation can contribute to visceral pain patterns.
🧫 Embryology (make it clinically relevant)
- Aortic arch derivatives: largely from pharyngeal arch arteries (key for congenital arch anomalies).
- Ligamentum arteriosum is the remnant of the ductus arteriosus and anchors the isthmus.
- Coarctation often occurs near the ductal region; collaterals develop via intercostals → classic rib notching.
📷 Anatomy images (keep)
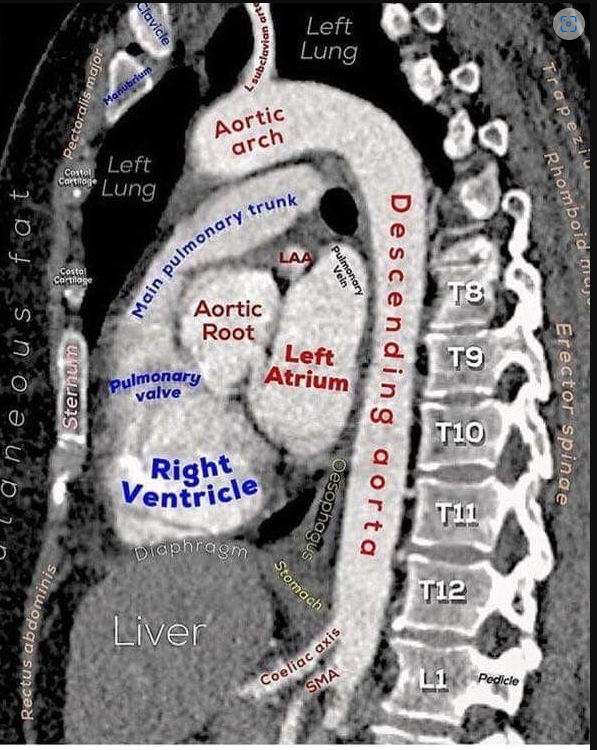
📸 Lateral Radiology (keep)
⚙️ Key functions (link anatomy to physiology)
- Oxygenated blood distribution: conduit from LV to all systemic beds.
- Pressure reservoir (Windkessel): elastin-rich media stores systolic energy → diastolic recoil.
- Pulse dampening: reduces pulsatile stress downstream; loss of compliance increases pulse pressure.
- Pulse wave velocity: rises as the aorta stiffens (ageing/atherosclerosis) and correlates with cardiovascular risk.
🧪 Imaging anatomy (what each modality shows best)
- Ultrasound: first-line for AAA screening and surveillance; best for diameter measurement.
- CT angiography: defines anatomy for operative planning (neck length, branch involvement) and dissection mapping.
- Chest X-ray: may show widened mediastinum/abnormal aortic contour (non-specific but important context).
- MRI/MRA: useful in selected cases; avoids ionising radiation.
🚨 Clinical relevance (retain, but tighten and anatomise)
- 🔴 Aortic aneurysm
- Most commonly abdominal (infrarenal), but can be thoracic/root.
- Risk factors: smoking, hypertension, atherosclerosis; connective tissue disorders (thoracic/root).
- Applied anatomy: infrarenal aneurysms relate to renal arteries (suprarenal involvement raises operative complexity).
- UK: men are invited for AAA screening in the year they turn 65 (England).
- 🩸 Aortic dissection
- Intimal tear → blood tracks into media → false lumen; branch vessels may be occluded (malperfusion).
- Stanford A involves ascending aorta; Stanford B does not involve ascending aorta.
- Applied anatomy: ascending involvement risks coronary ostia, aortic valve, and pericardial tamponade.
- 🍼 Coarctation
- Typically juxtaductal (near ligamentum arteriosum).
- Collateral circulation via intercostals → rib notching.
- Clinical: radio-femoral delay; upper limb HTN with lower limb hypotension.
- ⚖️ Aortic valve disorders
- Root/ascending aorta pathology can coexist with bicuspid aortic valve disease.
- Root dilation → regurgitation; calcific stenosis → LV pressure overload.
📝 Summary
The aorta is an elastic conduit and pressure reservoir whose anatomy maps directly to clinical presentations: root and ascending disease affects the valve/coronaries; arch disease can affect airway/oesophagus and the left recurrent laryngeal nerve; thoracic branches supply chest wall and viscera; abdominal branches follow a predictable pattern (CSI + paired laterals) before bifurcating at L4. A strong mental model of segments + branches + relations makes aneurysm, dissection, and coarctation far easier to recognise and localise.
📷 Anatomy (keep)
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery