Related Subjects:
|Wolff-Parkinson White syndrome (WPW) AVRT
|Lown Ganong Levine Syndrome AVRT
|Supraventricular Tachycardia (SVT)
|Atrioventricular Nodal Reentrant Tachycardia AVNRT
|Atrial Flutter
|Atrial Fibrillation
|Sinus Tachycardia
|Sinus Arrhythmia
|Multifocal Atrial Tachycardia
|Resuscitation - Adult Tachycardia Algorithm
📖 About
- Any tachycardia arising from above the level of the Bundle of His.
- Usually refers to reentrant tachycardias around the AV node (AVNRT).
- When the reentry pathway is beyond the node = AVRT (e.g., WPW, Lown-Ganong-Levine).
🧬 Aetiology of AVNRT
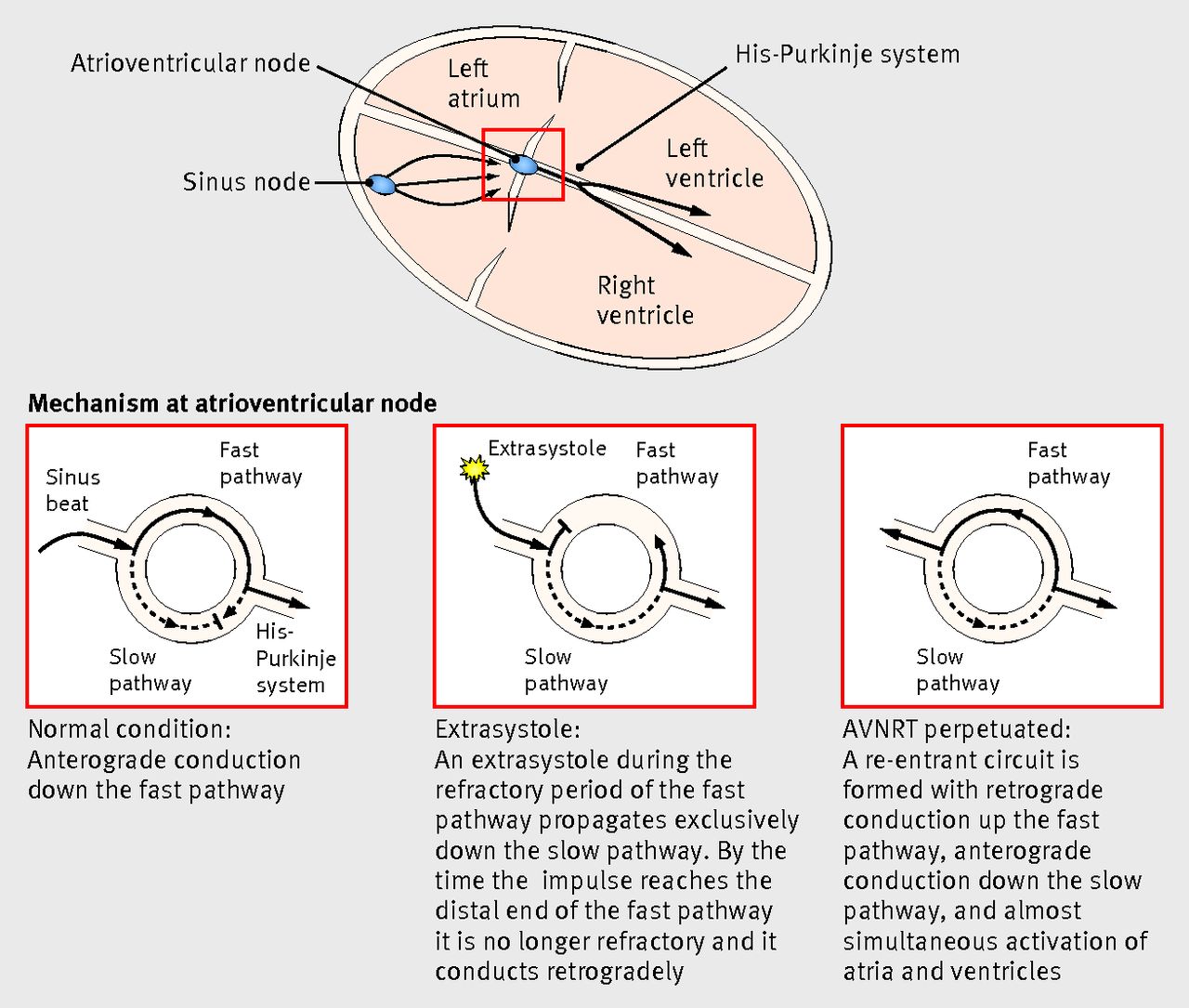
- Requires 2 pathways (dual physiology) around the AV node:
- ⚡ Slow pathway: short refractory period.
- ⚡ Fast pathway: long refractory period.
- An atrial ectopic impulse may travel down the slow and retrogradely up the fast pathway → like a “🎆 Catherine wheel firework”.
📊 Classification
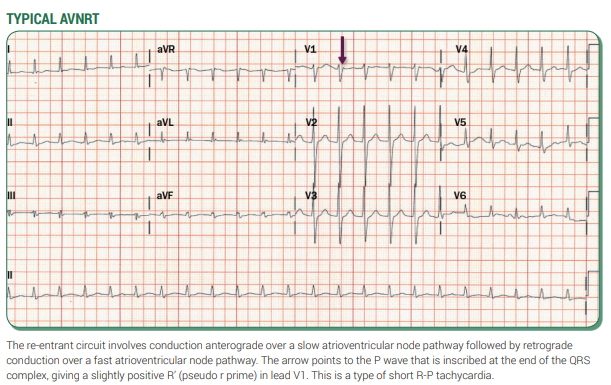
- 🔹 Slow–Fast (≈90%, RP′ < P′R).
- 🔹 Fast–Slow (≈10–15%, RP′ > P′R).
- 🔹 Slow–Slow (<5%).
🖼️ Diagram showing AVNRT
 🩺 Clinical
🩺 Clinical
- Occurs at any age; benign; more common in young females (2:1 ratio).
- Symptoms: palpitations, presyncope, breathlessness, dizziness, chest pain.
- Can be misdiagnosed as a panic attack (often delayed diagnosis).
- Triggers: stress, caffeine, alcohol, smoking, drugs.
🔍 Investigations
- Bloods: FBC, U&E, TFTs, LFTs. CXR.
- 12-lead ECG during episode: narrow complex tachycardia 120–240 bpm. May mimic VT if bundle branch block present.
- Implantable loop recorder if transient/undocumented episodes.
- Echo: exclude structural disease.
- Rarely: check for phaeochromocytoma if hypertension present.
💡 Clinical Pearls
- ⚡ Sudden onset/offset → suggests PSVT.
- 👔 “Shirt flapping” or “neck pounding” → highly suggestive of AVNRT.
- 🚨 Hypotension/syncope → poorly tolerated → urgent treatment/referral.
- Structural heart disease → consider atrial tachycardia.
- Pre-excitation (AVRT/WPW) → refer for specialist ablation.
📸 Examples
 💊 Management
💊 Management
- 🛑 If unstable → immediate DC cardioversion.
- Stable:
- ✅ Vagal manoeuvres (Valsalva, carotid sinus massage).
- ✅ IV adenosine (6–24 mg rapid bolus). Warn about transient unpleasant sensations.
- ✅ IV verapamil (2.5–5 mg slow IV) or diltiazem (if narrow complex only).
- ⚠️ If broad-complex SVT (aberrancy or accessory pathway) → get urgent expert advice. Avoid verapamil/diltiazem if pre-excited AF suspected.
- Pre-excited AF (AVRT): avoid AV nodal blockers (adenosine, digoxin, β-blockers, calcium blockers). Use IV flecainide/propafenone/amiodarone or cardioversion if unstable.
- 📅 Long-term: refer to electrophysiology for catheter ablation (high cure rates, low risk).
📚 References
Cases - AVNRT with Acute Management
- Case 1 - Young Woman with Palpitations:
A 26-year-old woman presents to A&E with sudden-onset palpitations, HR 180 bpm, BP 120/70, regular narrow-complex tachycardia on ECG.
Management: She is stable → start with modified Valsalva manoeuvre (reverts to sinus rhythm). Observe and discharge with cardiology follow-up. Education on avoiding triggers (caffeine, alcohol).
- Case 2 - Middle-aged Man with Dizziness:
A 48-year-old man arrives with palpitations and dizziness. HR 170 bpm, BP 115/70, regular narrow-complex tachycardia. Vagal manoeuvres fail.
Management: Give adenosine IV 6 mg rapid bolus → no effect. Repeat 12 mg → tachycardia terminates, sinus rhythm restored. Monitor in ED, advise GP/cardiology follow-up. If recurs frequently → consider prophylaxis or ablation.
- Case 3 - Elderly Patient with Chest Pain and Hypotension:
A 70-year-old woman with history of hypertension presents with palpitations, chest pain, and lightheadedness. HR 190 bpm, BP 80/50. ECG: narrow-complex tachycardia.
Management: She is unstable → immediate synchronised DC cardioversion. Once stabilised, admitted under cardiology, plan for further evaluation and long-term management (beta-blocker vs catheter ablation depending on comorbidities).
Teaching Commentary ⚡
These three cases highlight the spectrum:
- Stable + young → vagal manoeuvres often suffice.
- Stable but symptomatic → escalate to adenosine, with verapamil or beta-blocker as alternatives.
- Unstable → don’t delay: immediate DC cardioversion.
Always remember adenosine is contraindicated in asthma/COPD and should be avoided in patients on dipyridamole or with transplanted hearts (increased sensitivity). Long-term, radiofrequency ablation of the slow pathway is curative in most patients.
