
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Anatomy and Physiology of the Thyroid Gland
Related Subjects: |Thyrotoxicosis and Hyperthyroidism |Thyroid Storm - Thyrotoxic crisis |Graves Disease (Thyrotoxicosis) |Amiodarone and Thyroid disease |Thyroid Surgery (Thyroidectomy) |Hypothyroidism |Hashimoto's thyroiditis |DeQuervain's thyroiditis |Subacute Thyroiditis |Thyroid nodule |Congenital Hypothyroidism |Thyroid Function Tests and antibodies |Post partum thyroiditis |Sick Euthyroid Syndrome |Thyroid Exam (OSCE) |AP of the Thyroid |Thyroid Cancer
🦋 The thyroid “trap” refers to active iodide uptake into follicular cells via the sodium–iodide symporter (NIS) on the basolateral membrane (ATP-dependent indirectly via the Na⁺/K⁺-ATPase gradient). Iodide is then moved into the follicular lumen (colloid), where thyroglobulin (a large protein rich in tyrosine residues) is iodinated by thyroid peroxidase (TPO) to form thyroid hormones. The thyroid gland is a vital endocrine organ producing T4 (thyroxine) and T3 (triiodothyronine), which regulate basal metabolic rate, thermogenesis, cardiovascular tone, and are essential for brain development and growth.
📍 Anatomy of the Thyroid Gland
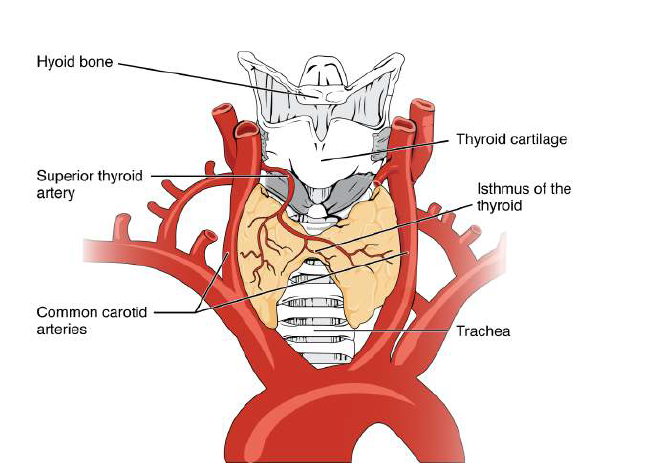
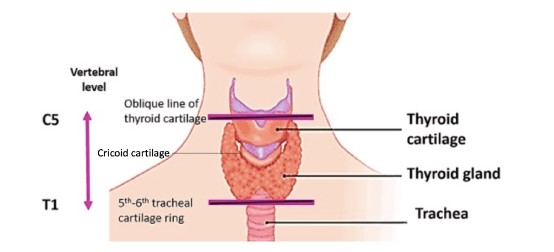
- Location: Anterior neck, typically spanning C5–T1, lying anterolateral to the upper trachea and inferior to the thyroid cartilage (“Adam’s apple”).
- Shape: Two lateral lobes connected by an isthmus (usually over the 2nd–4th tracheal rings). A pyramidal lobe may be present (thyroglossal tract remnant).
- Capsules:
- True capsule (fibrous, adherent to gland).
- False capsule (pretracheal fascia) - provides attachments; explains movement on swallowing.
- Key relations (surgical importance):
- Anterior: strap muscles (sternohyoid, sternothyroid, omohyoid).
- Medial: larynx, trachea, pharynx/oesophagus (oesophagus more left-sided posteriorly).
- Posterior: parathyroid glands (typically 4), and the recurrent laryngeal nerve in the tracheo-oesophageal groove.
- Superior pole: close to the external branch of the superior laryngeal nerve (voice pitch/cricothyroid).
- Histology:
- Follicles lined by follicular epithelial cells; lumen contains colloid (thyroglobulin storage depot).
- Parafollicular (C) cells between follicles secrete calcitonin (minor role in adult calcium homeostasis; marker in medullary thyroid carcinoma).
🩸 Blood Supply, Lymphatics & Innervation
- Arterial supply:
- Superior thyroid artery (from external carotid).
- Inferior thyroid artery (from thyrocervical trunk).
- Thyroidea ima artery (variant, from brachiocephalic trunk/aorta) - important in surgery/bleeding risk.
- Venous drainage: Superior + middle thyroid veins → internal jugular; inferior thyroid veins → brachiocephalic veins.
- Lymphatics: Prelaryngeal (Delphian), pretracheal, paratracheal → deep cervical nodes (relevant in thyroid cancer spread).
- Innervation: Sympathetic fibres from cervical ganglia regulate vascular tone; hormone output is primarily regulated hormonally by TSH, not direct neural stimulation.
🧪 Thyroid Hormone Synthesis (Step-by-step)
Think of thyroid hormone production as: trap iodide → move into colloid → oxidise/organify → couple → store → retrieve → release. The gland uniquely stores weeks’ worth of hormone in the colloid, which is why onset/offset of thyroid disease and treatment can be slow.
- 1) Iodide uptake (“trapping”): I⁻ enters follicular cells via NIS (Na⁺/I⁻ symporter) on the basolateral membrane.
- Stimulated by: TSH.
- Inhibited by: high iodide load (acute Wolff–Chaikoff effect), some anions (perchlorate/thiocyanate).
- 2) Apical transport into colloid: I⁻ exits into follicular lumen via pendrin (apical iodide transporter).
- Clinical link: Pendrin defects can cause goitre with sensorineural deafness (Pendred syndrome).
- 3) Thyroglobulin (Tg) production: Follicular cells synthesise Tg and secrete it into the colloid (protein scaffold for hormone synthesis and storage).
- 4) Oxidation & organification (TPO-dependent):
- Thyroid peroxidase (TPO) oxidises iodide and iodinates tyrosine residues on Tg → forms MIT and DIT.
- This step requires hydrogen peroxide generation (a key metabolic step; relevant to oxidative stress and autoimmunity concepts).
- Drug link: Thionamides (carbimazole/methimazole, PTU) inhibit TPO (organification + coupling).
- 5) Coupling (TPO-dependent):
- MIT + DIT → T3
- DIT + DIT → T4
- Hormone remains bound to Tg in colloid as a storage form.
- 6) Endocytosis & proteolysis (TSH-stimulated):
- Colloid is endocytosed; lysosomal proteolysis releases T4 and T3 from Tg.
- MIT/DIT recycling: Deiodinase enzymes reclaim iodide from MIT/DIT (iodide conservation).
- 7) Secretion & transport in blood:
- T4/T3 exit to circulation; most is protein-bound (mainly TBG, also transthyretin and albumin).
- Free fraction is biologically active; lab “free T4/T3” reflects this.
🔄 Peripheral Conversion & Why T3 Matters
The thyroid secretes mostly T4, which acts as a prohormone. In tissues, deiodinases convert T4 → T3 (active) or → reverse T3 (inactive). This “local activation” lets organs fine-tune thyroid signalling depending on illness, nutrition, and stress.
- Deiodinase types:
- D1/D2: generate active T3 (liver, kidney, brain, pituitary, muscle).
- D3: generates reverse T3 (protective down-regulation; rises in critical illness).
- Clinical link: “Non-thyroidal illness” can show low T3 ± low/normal T4 with inappropriately normal/low TSH (interpret TFTs cautiously in acute illness).
🎛 Regulation: Hypothalamic–Pituitary–Thyroid (HPT) Axis
- Hypothalamus: TRH → stimulates pituitary thyrotrophs.
- Pituitary: TSH → stimulates:
- NIS iodide uptake
- TPO activity and coupling
- Tg synthesis
- Endocytosis/proteolysis of colloid
- Growth/trophic effects on follicular cells (chronic TSH stimulation → goitre)
- Negative feedback: Free T3/T4 inhibit TRH and TSH (pituitary is very T3-sensitive due to local conversion).
- Other modulators: Dopamine and somatostatin can suppress TSH; cold exposure increases TRH (more prominent in neonates).
🔥 Actions of Thyroid Hormones (Mechanism → Effects)
T3 enters cells and binds nuclear thyroid hormone receptors, altering gene transcription. It increases mitochondrial activity and upregulates proteins such as Na⁺/K⁺-ATPase, driving oxygen consumption and heat production. Many “hyperthyroid” features reflect increased tissue responsiveness to catecholamines (via β-adrenergic upregulation), not simply high hormone levels alone.
- Metabolic: ↑ basal metabolic rate, ↑ thermogenesis, ↑ lipolysis, ↑ carbohydrate turnover; lowers LDL by increasing LDL receptor expression.
- Cardiovascular ❤️: ↑ heart rate and contractility, ↑ cardiac output, ↓ systemic vascular resistance (warm peripheries). Can precipitate AF, angina, or heart failure in susceptible patients.
- Respiratory: ↑ ventilatory drive; in severe thyrotoxicosis, respiratory muscle weakness can contribute to breathlessness.
- CNS 🧠: alertness, mood, reaction speed; excess → anxiety/irritability/insomnia; deficiency → slowing, low mood.
- Growth & development 👶: essential for neuronal migration, myelination, synaptogenesis; deficiency in early life risks irreversible neurodevelopmental impairment.
- Muscle/bone: excess → proximal myopathy and ↑ bone turnover (osteoporosis risk); deficiency → myalgia, stiffness, delayed reflex relaxation.
- GI: ↑ gut motility (diarrhoea in hyperthyroidism; constipation in hypothyroidism).
- Reproductive: menstrual disturbance, subfertility; pregnancy alters binding proteins and reference ranges (interpret TFTs with trimester-specific ranges).
🧪 Thyroid Function Tests (How to Think About Them)
- TSH: most sensitive screening marker (log-linear response to free T4). However, may be misleading in pituitary disease or severe non-thyroidal illness.
- Free T4: best reflection of circulating hormone availability; primary marker of severity in overt hypothyroidism/hyperthyroidism.
- Free T3: useful when hyperthyroidism suspected with borderline T4 (T3-toxicosis).
- Autoantibodies:
- Anti-TPO (± anti-thyroglobulin): autoimmune thyroid disease (Hashimoto’s most typical).
- TSH receptor antibodies (TRAb/TSI): Graves’ disease; also relevant in pregnancy/neonatal risk assessment.
- Calcitonin: not routine for function; tumour marker for medullary thyroid carcinoma in selected contexts.
🏥 Clinical Relevance (High-Yield Patterns)
- Hypothyroidism:
- Symptoms/signs: fatigue, weight gain, cold intolerance ❄️, constipation, dry skin, bradycardia, hoarse voice, delayed reflexes.
- Typical labs: ↑ TSH, ↓ free T4 (primary); in secondary (pituitary), TSH low/normal with low T4.
- Common causes: Hashimoto’s, post-thyroidectomy/radioiodine, iodine deficiency (global), drugs (amiodarone, lithium).
- Hyperthyroidism / thyrotoxicosis:
- Symptoms/signs: weight loss, heat intolerance ☀️, tremor, palpitations, anxiety, diarrhoea, proximal weakness.
- Typical labs: ↓ TSH with ↑ free T4 and/or ↑ T3.
- Common causes: Graves’, toxic multinodular goitre, toxic adenoma; thyroiditis can cause “leak” thyrotoxicosis (often low uptake on scans).
- Emergency: thyroid storm = life-threatening hypermetabolic state (fever, delirium, tachyarrhythmia) requiring urgent hospital management.
- Goitre & nodules:
- Goitre reflects chronic stimulation (TSH, TRAb) or dyshormonogenesis; assess compressive symptoms (stridor, dysphagia) and malignancy risk features.
- Thyroid nodules are common; most are benign, but require risk stratification and ultrasound-led assessment.
📝 Summary
The thyroid is a highly vascular endocrine gland whose follicles uniquely store hormone precursor in colloid. Thyroid hormone synthesis relies on iodide trapping by NIS, apical transport via pendrin, and TPO-mediated organification and coupling on thyroglobulin to form T3/T4, followed by TSH-driven retrieval and release. Most circulating hormone is protein-bound; tissue deiodinases convert T4 into active T3, enabling organ-specific control. Clinically, TFT interpretation hinges on physiology: TSH is sensitive for primary disease, while acute illness and pituitary dysfunction can distort the expected axis response.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery