
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Small vessel disease
Related Subjects: |Neurological History taking |Causes of Stroke |Ischaemic Stroke |Subarachnoid Haemorrhage |Small Vessel Disease |Vascular Dementia |Dementias |CADASIL |CARASIL |Cerebral Arterial Perfusion and Clinical Correlates |Anterior circulation Brain |Posterior circulation Brain |Acute Stroke Assessment (ROSIER&NIHSS) |Carotid Artery dissection |Vertebral artery dissection |Acute Stroke Assessment (ROSIER&NIHSS) |Atrial Fibrillation |Atrial Myxoma |Causes of Stroke |Ischaemic Stroke |Cancer and Stroke |Cerebral Venous thrombosis |Cardioembolic stroke |CT Basics for Stroke |Endocarditis and Stroke |Haemorrhagic Stroke |Stroke Thrombolysis |Hyperacute Stroke Care |AP of the Brain |Cryptogenic stroke |Carotid Web |Anterior / Medial Medullary Infarct (Dejerine Syndrome)
🧠 Introduction
- Cerebral Small Vessel Disease (SVD) causes ~25% of all ischaemic strokes and >40% of dementia cases.
- It contributes to cognitive decline, gait impairment, mood disturbance, and vascular dementia.
- Common in the elderly on CT/MRI, but imaging–clinical correlation is variable (asymptomatic → gait dyspraxia → dementia).
- Underlying pathology for many deep haemorrhages (see haemorrhagic stroke chapter).
- Strongly linked to hypertension and other vascular risk factors.
- SVD itself cannot be directly imaged - instead, we use markers: lacunes, microbleeds, WMHs.
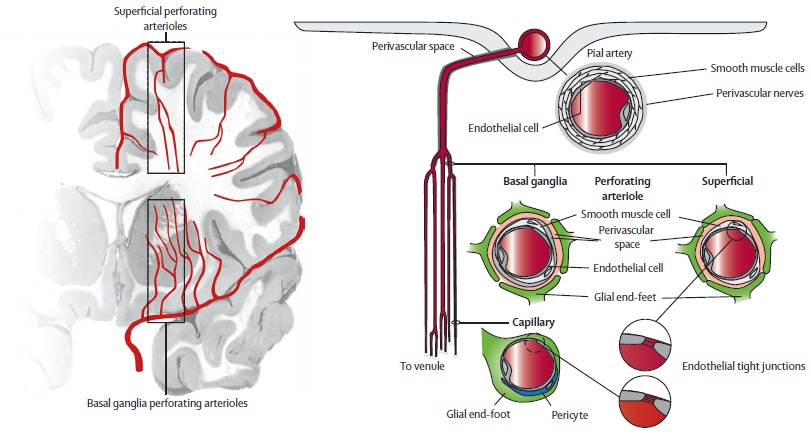
⚙️ Aetiology & Pathology
- A disease of small penetrating arterioles (<800 µm), branching from the Circle of Willis and vertebrobasilar system.
- Exposed to high pressures → prone to injury.
- Key mechanisms:
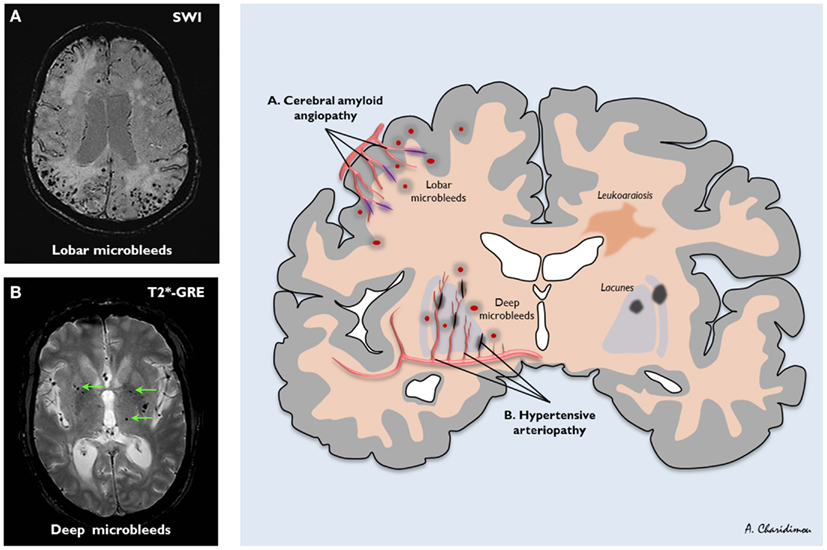
- 🩸 Lipohyalinosis (degenerative, different to atherosclerosis).
- 🧠 Amyloid angiopathy (elderly, lobar bleeds).
- 🧬 Inherited genetic defects (CADASIL, Fabry’s, CARASIL).
- 🦠 Vasculitis (autoimmune/inflammatory).
- End result → white matter demyelination, axonal loss, gliosis, and small deep strokes (lacunes <15 mm).
- Risk factors: age, hypertension, diabetes.
💡 Clinical pearl: Multiple acute lacunar infarcts → think embolism (not pure SVD).
🔬 Imaging Features
- CT: Periventricular hypodensity, often with atrophy.
- MRI T2/FLAIR: White matter hyperintensities (WMHs) in periventricular & deep regions.
- DWI: Detects acute lacunes (≤1.5 cm).
- Gradient echo / SWI: Microbleeds (siderosis).
- Appearance can mimic demyelination (MS).
📏 Fazekas Scale
Grades WMHs severity:
PVWM 0–3 (caps → halo → extension) and DWM 0–3 (punctate → confluent).
Used more in research than routine practice.
🧩 Clinical Spectrum
- Often subclinical, but may present as:
- Classical lacunar syndromes:
- Pure motor or pure sensory stroke.
- Sensorimotor stroke.
- Ataxic hemiparesis.
- Dysarthria–clumsy hand.
- Hemichorea / hemiballismus.
- Chronic manifestations: Vascular dementia, gait apraxia, vascular parkinsonism.
📚 Pantoni’s Classification (2010)
SVD is heterogeneous - multiple pathologies converge on small vessels:
- 🩸 Arteriosclerosis: Lipohyalinosis, microaneurysms (HTN, diabetes, age).
- 🧠 Amyloid angiopathy: β-amyloid deposition, lobar bleeds, Alzheimer link.
- 🧬 Inherited: CADASIL, CARASIL, Fabry’s, MELAS, COL4A1 mutations.
- 🦠 Vasculitis/Immune: SLE, RA, ANCA vasculitides, Sneddon’s syndrome.
- Other: post-radiation angiopathy, venous collagenosis.
🩺 Management
- No specific cure - focus is on risk factor modification.
- 🎯 Control hypertension, diabetes, lipids, smoking.
- 💊 Antiplatelet therapy: Aspirin first-line. SPS3 trial: no benefit of dual therapy (aspirin+clopidogrel).
- 🏃 Lifestyle: exercise, diet, vascular prevention.
- 🔍 Consider genetic causes if young onset (e.g. CADASIL, Fabry’s).
- In acute stroke → thrombolysis is not contraindicated in lacunar infarction.
💡 Exam Pearl: SVD is the main cause of lacunar stroke, vascular dementia, gait apraxia, and deep haemorrhage. Think “small deep vessel” whenever you see a lacunar infarct on CT/MRI.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery