
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Acute Pericarditis ✅
Related Subjects: | Assessing Breathlessness | Assessing Chest Pain | Pericardial Effusion and Tamponade | Constrictive Pericarditis | Colchicine |Acute Coronary Syndrome (ACS) General |Aortic Dissection |Pulmonary Embolism |Acute Pericarditis |Diffuse Oesophageal Spasm |Gastro-oesophageal reflux |Oesophageal Perforation Rupture |Pericardial Effusion Tamponade
❤️ Acute pericarditis = inflammation of the pericardial sac. Classic ECG: widespread concave (“saddle-shaped” ⛰️) ST elevation + PR depression 📉. Presentation ranges from mild chest pain to tamponade or myopericarditis.
🌍 Epidemiology
- ~5% of chest pain presentations in the ED 🏥
- Complications (tamponade, constriction) occur in ~5%
- Most common in young adults (viral/post-viral)
🩺 Clinical Features
- Sharp, pleuritic chest pain ❤️🔥 (worse lying down, improves sitting forward 🪑)
- Fever 🤒, malaise, myalgia
- Pericardial rub 🎧: 3 components, squeaky at LSB
- Distant heart sounds → suggestive of effusion 💧
- Dyspnoea if effusion or tamponade
- Assess for tamponade: raised JVP, hypotension, pulsus paradoxus >10–15 mmHg 🚨
❓ Differential Diagnosis
- Acute coronary syndrome (MI) ❤️🔥
- Myocarditis 🫀
- Aortic dissection 🌪️
- Pneumonia 🌬️, pulmonary embolism 🩸
- Gastroesophageal pain 🍔🔥
- Musculoskeletal pain 💪
🧬 Causes
| Category | Examples | Notes / Investigations |
|---|---|---|
| Idiopathic / Post-viral | Coxsackie, Adenovirus, Influenza | Most common; diagnosis of exclusion. Mild CRP rise, ECG typical ST/PR changes. |
| Post-MI (Dressler’s) | Autoimmune response 2–6 weeks post-MI | Fever, rub, effusion; elevated ESR/CRP; troponin normal/mild rise. |
| Post-pericardiotomy | After cardiac surgery | Often mild, self-limiting; monitor for effusion. |
| Bacterial / Fungal / TB | Staph, Strep, TB, Candida | Blood cultures, pericardial fluid analysis, PCR for TB, echo/CT for effusion. |
| Malignancy | Lung, breast, lymphoma | Pericardial effusion ± tamponade; cytology of fluid, imaging for tumour. |
| Metabolic / Uraemic | CKD, dialysis | High BUN/creatinine; ECG +/- effusion; treat underlying renal failure. |
| Autoimmune | SLE 🦋, RA, scleroderma | ANA, dsDNA, inflammatory markers; treat flare with immunosuppression. |
| Trauma / Radiation / Drugs | Radiotherapy, chemotherapy, medications | History key; ECG, echo, inflammatory markers; stop offending drug if possible. |
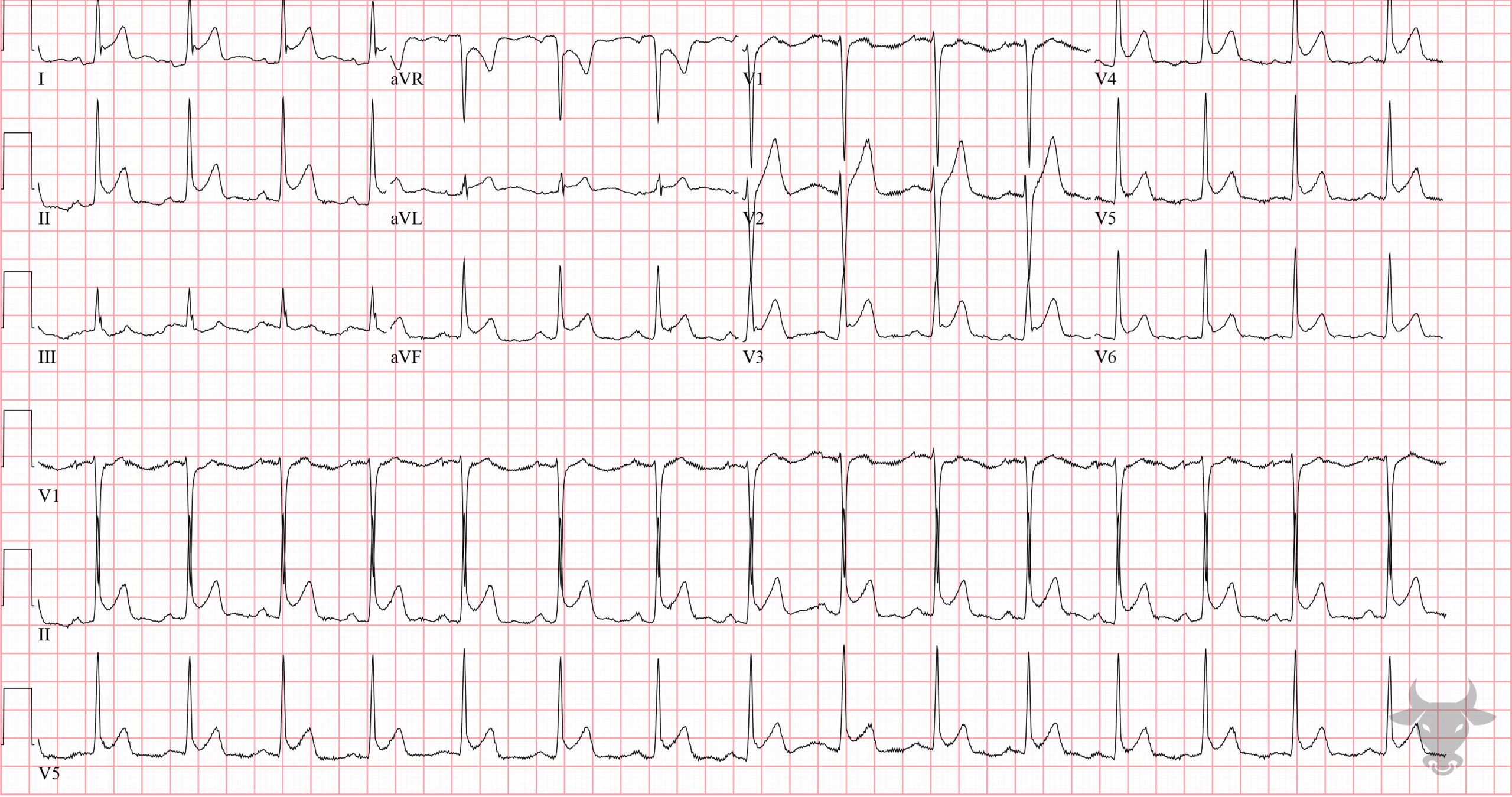
🩺 ECG Changes in Acute Pericarditis: The hallmark ECG pattern is widespread concave (“saddle-shaped”) ST-segment elevation accompanied by PR-segment depression in most leads (except aVR, which may show PR elevation). The changes typically evolve through four stages:
1️⃣ Stage 1: Acute – widespread ST elevation + PR depression (hours to days).
2️⃣ Stage 2: ST and PR segments begin to normalize.
3️⃣ Stage 3: T-wave inversion develops once ST segments normalize.
4️⃣ Stage 4: ECG gradually returns to baseline.
Other features may include low-voltage QRS if there is pericardial effusion and transient arrhythmias. Unlike STEMI, the ST elevation in pericarditis is diffuse and concave rather than localized and convex, and reciprocal changes are generally absent. Serial ECGs are recommended to monitor evolution and detect complications.
 🔎 Investigations
🔎 Investigations
- Bloods: FBC, U&E, CRP/ESR ↑, troponin if myopericarditis
- ECG: 4 stages – 1️⃣ widespread concave ST ↑ + PR ↓, 2️⃣ normalization, 3️⃣ T inversion, 4️⃣ T wave normalization
- CXR: usually normal; ± cardiomegaly if effusion
- Echocardiography: assess effusion, tamponade, LV function
- Cardiac MRI: myocardial inflammation, edema (Lake Louise criteria)
- Pericardial fluid analysis: cytology, culture, TB PCR if effusion present
- Autoimmune/serology as indicated (ANA, dsDNA, RF, viral serologies)
📊 Prognostic Predictors
- Major: Fever >38°C, CRP elevation, subacute onset, large effusion, tamponade, NSAID non-response
- Minor: Immunosuppression, trauma, anticoagulants, myopericarditis
🩺 Management (NICE-compliant)
- Bed rest 🛌 until symptom resolution, avoid strenuous exercise until CRP, ECG, echo normalize (≥3 months for athletes)
- First-line pharmacologic: NSAID (e.g., Ibuprofen 400–600mg TDS) + PPI prophylaxis
- Colchicine 0.5–1 mg/day for 3 months to reduce recurrence
- Second-line: Low-dose corticosteroids if NSAID/colchicine contraindicated (exclude infection first)
- Recurrent pericarditis: escalate to IVIG 💉, Anakinra 🧬, or azathioprine 💊 if steroid-dependent or refractory
- Severe / life-threatening effusion: pericardiocentesis or pericardiectomy 🛠️
- Infective pericarditis: targeted antibiotics/antifungals/anti-TB therapy
- Neoplastic pericarditis: oncology referral, chemo/radiotherapy as indicated
- Post-MI (Dressler): NSAIDs + colchicine; avoid anticoagulants if large effusion
- Uraemic pericarditis: intensify dialysis; NSAIDs with caution; colchicine if tolerated
- Monitor: ECG, CRP, echo; treat complications (tamponade, arrhythmia) promptly
📚 References / Guidelines
- 2015 ESC Guidelines on Pericardial Disease
- NICE Clinical Knowledge Summary – Chest Pain
- Adler Y et al. Eur Heart J. 2015;36:2921–2964
🧑⚕️ Case Examples - Acute Pericarditis
- Case 1 (Viral): 🦠 25-year-old man with pleuritic chest pain relieved sitting forward. ECG: widespread ST elevation + PR depression. CRP mildly raised. Management: NSAID + colchicine, rest, monitor for effusion.
- Case 2 (Post-MI Dressler’s): ❤️🔥 60-year-old man, 3 weeks post-STEMI, fever, pericardial rub, effusion. Management: NSAID + colchicine, avoid anticoagulation if large effusion, monitor echo.
- Case 3 (Uraemic): 🧬 48-year-old man with CKD5 on dialysis, chest pain, pericardial rub, small effusion. Management: Intensify dialysis, cautious NSAID/colchicine, monitor for tamponade.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery