🧠 The classic presentation of an Extradural Haematoma (EDH) is:
➡️ Head injury → brief loss of consciousness → lucid interval → rapid decline in GCS.
🚨 This is a neurosurgical emergency requiring urgent CT imaging and intervention.
💡 About
- EDH = bleeding between the dura mater and skull, confined by the skull’s periosteal suture lines.
- Classically arterial, most often from the middle meningeal artery.
- Rapidly progressive → may cause brain herniation if untreated.
- Accounts for ~2% of head injuries, typically in young adults (20–30 years), often after high-impact trauma.
🔎 Aetiology & Causes
- Rupture of the middle meningeal artery (or vein).
- Associated with temporal/parietal skull fractures.
- Common causes:
- Falls 🪂
- Road traffic collisions 🚗
- Assaults 🥊
- Sports injuries (e.g., skiing) ⛷️
- Rarely: birth trauma in neonates 👶
🩺 Clinical Features
- Initial head trauma ± scalp wound.
- Lucid interval → temporary recovery → rapid neurological deterioration.
- ↓ GCS, confusion, drowsiness, then coma.
- Focal neurology (e.g., hemiparesis, dilated ipsilateral pupil from CN III palsy).
- Raised ICP signs: Cheyne–Stokes respiration, bradycardia, hypertension (Cushing’s triad).
🧪 Investigations
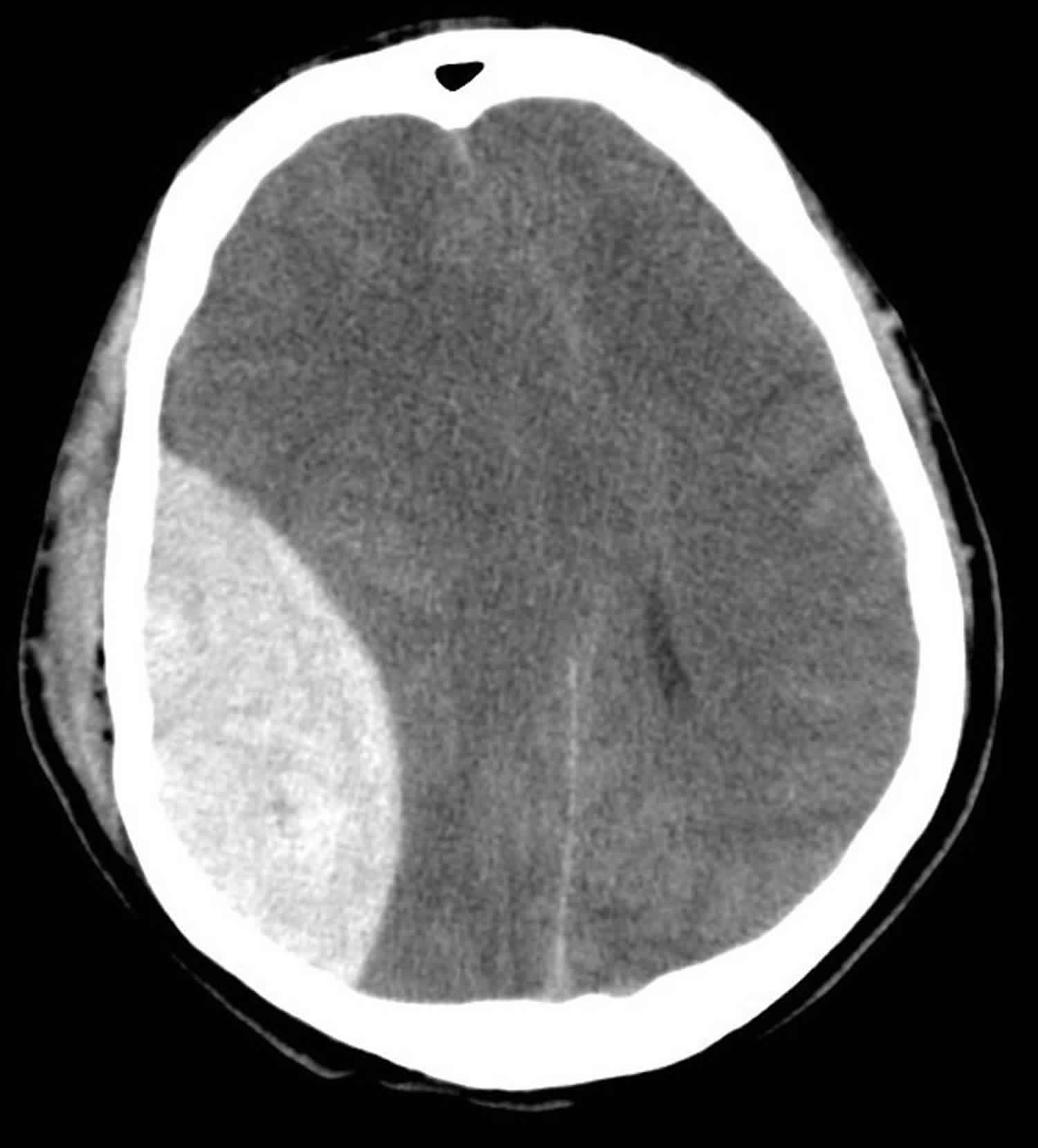
- CT Head (Gold Standard):
- Biconvex (lens-shaped) hyperdense lesion.
- Confined by suture lines (unlike subdural haematoma).
- May show midline shift ± skull fracture.
- Bloods: FBC, U&E, LFTs, clotting screen (relevant if anticoagulated).
⚡ Management
- Initial ABC resuscitation: Secure airway, give O₂, IV fluids. Intubate if GCS < 8.
- Urgent neurosurgical referral in all suspected cases.
- Reverse coagulopathy (vitamin K, PCC if on warfarin; stop antiplatelets if safe).
- Surgery:
- Immediate evacuation indicated if clot >30 cm³, thickness >15 mm, midline shift >5 mm, or GCS ≤8 with focal deficit.
- Craniotomy = definitive treatment.
- Burr hole may be lifesaving if deterioration occurs before theatre access.
- Post-operative: ICU care with ICP monitoring, neuro-rehab as required.
📋 Key Exam Tips
✅ Lucid interval is the buzzword for EDH (but not always present).
✅ CT: biconvex/lens-shaped bleed, confined by sutures.
✅ Differentiate from Subdural Haematoma (crescent-shaped, not limited by sutures).
✅ Always think middle meningeal artery rupture in temporal fracture.
