
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Anatomy and Physiology of the Spine
Related Subjects: |AP of the Spinal Cord |AP of the Spine |Initial Trauma Assessment and Management |Cervical Spine Immobilization and Management |Trauma: Spinal Injury
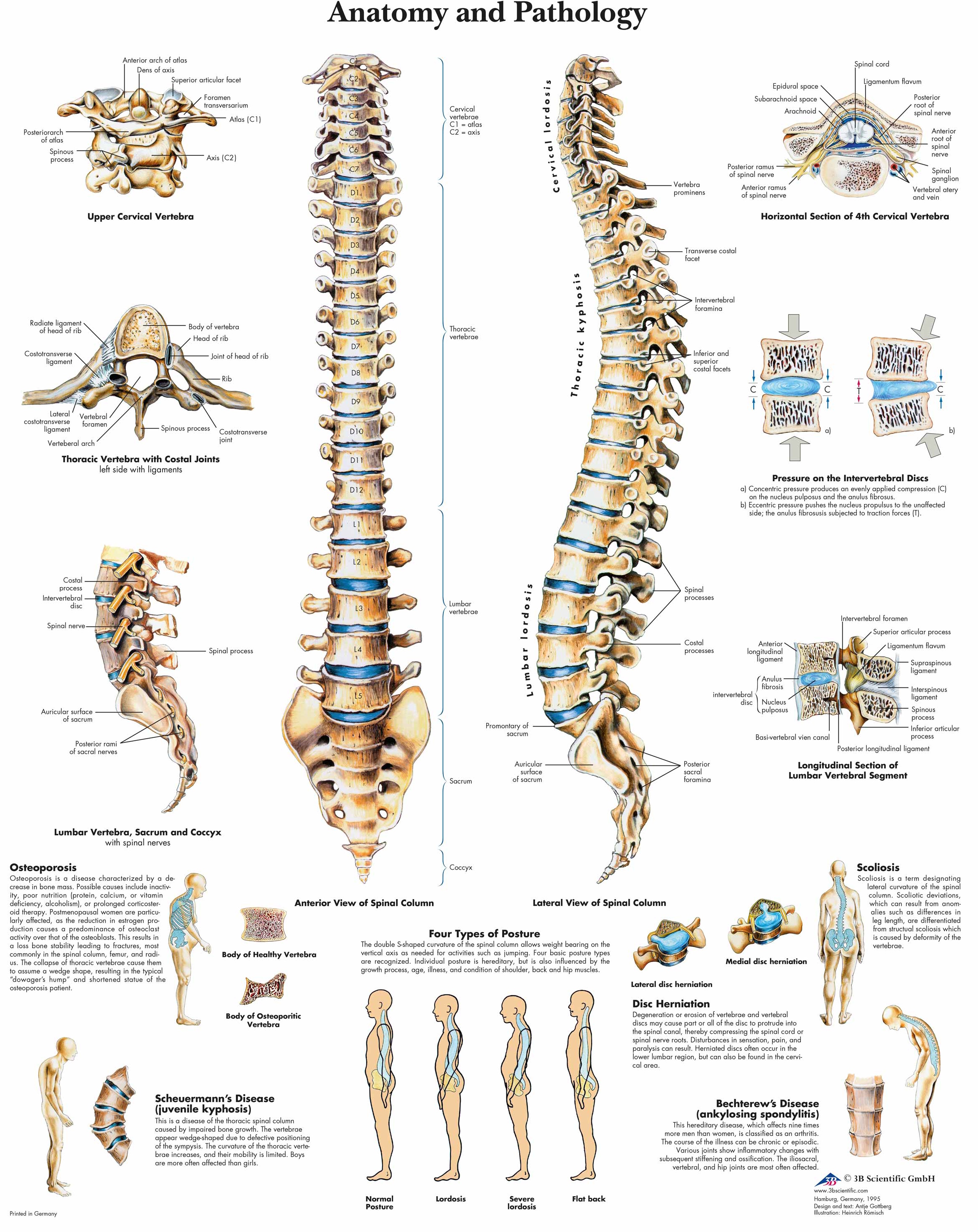
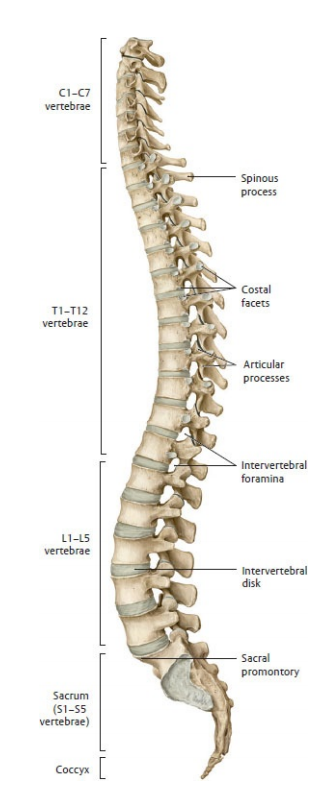
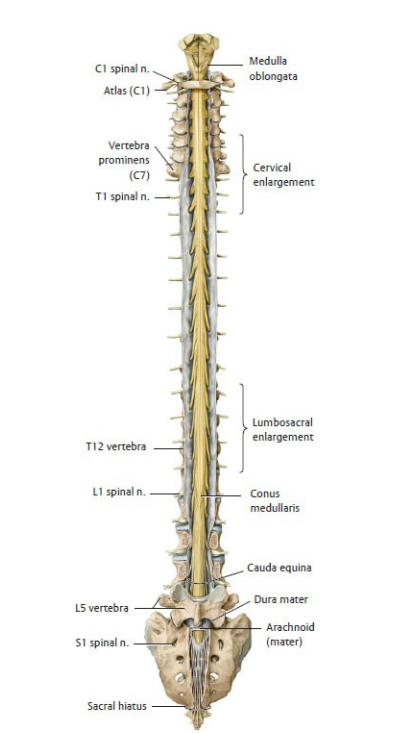
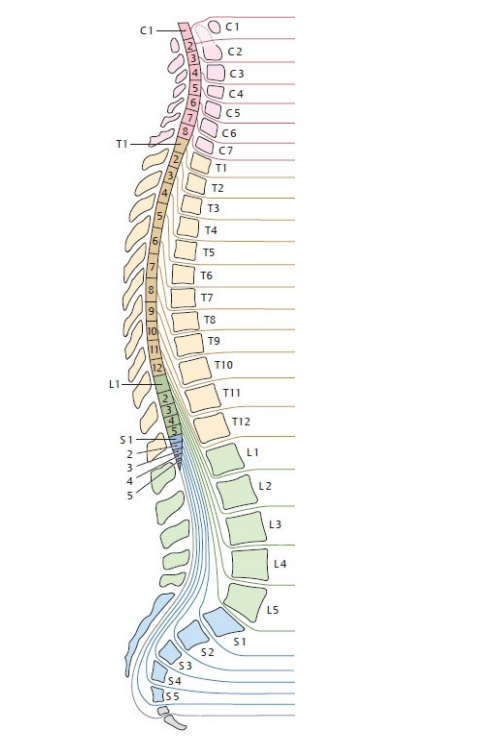
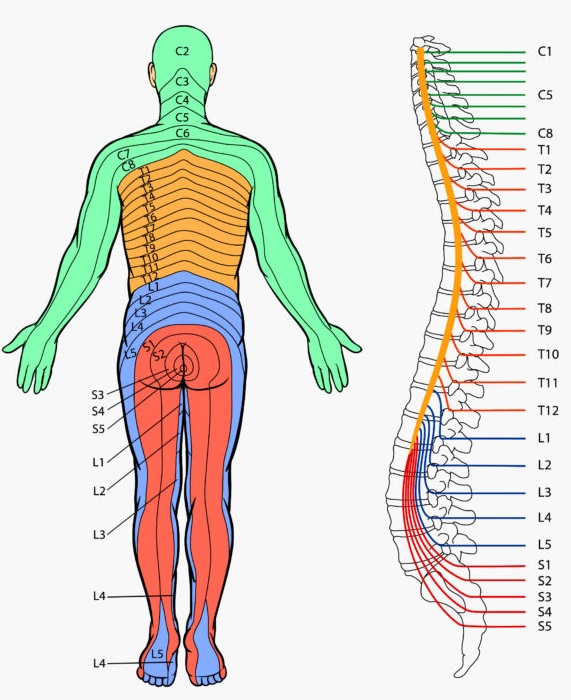
🦴 The spine (vertebral column) is a segmented, load-bearing “mast” made of bone, joints, discs and ligaments: it must be stiff enough to transmit load yet mobile enough to position the head and trunk. Inside it, the spinal cord is CNS tissue (upper motor neurone pathways + autonomics) that ends as the conus medullaris around L1–L2 in adults; below this, the canal contains the cauda equina (lumbosacral nerve roots floating in CSF), which behave like peripheral nerves/LMNs. A key “gotcha” is that cord segments don’t sit at the same vertebral level: vertebral trauma/tumour at (say) T12 can injure higher cord segments, whereas lumbar canal disease often compresses roots rather than cord.
Cervical Region
Thoracic Region
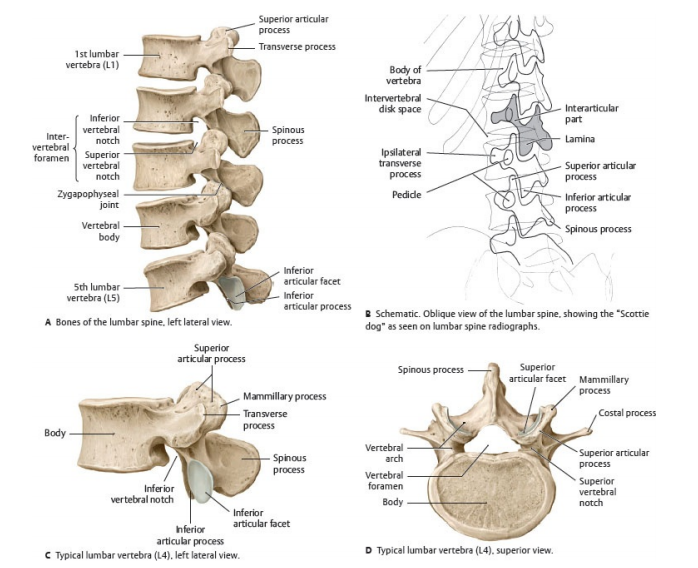
Lumbar Region
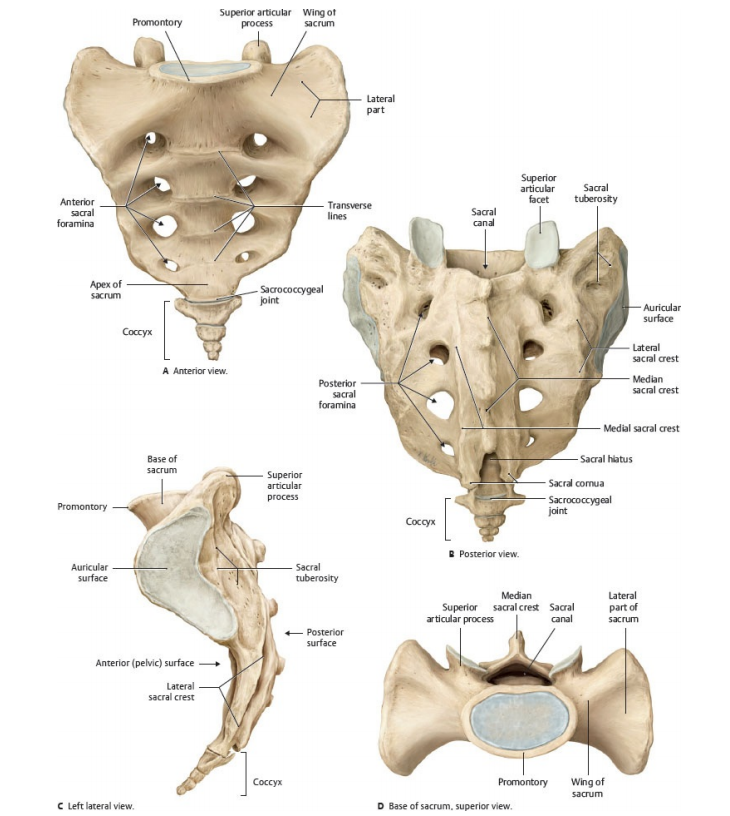
Sacral Region
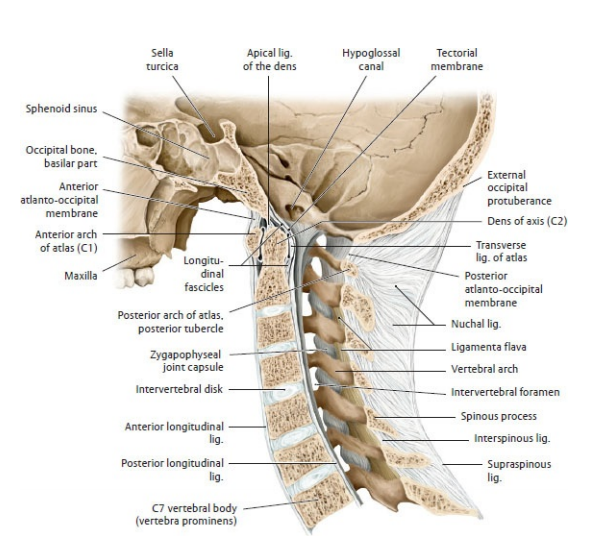
Skull and Atlas-Axis Relationship
Spinal Cord Anatomy
Spinal Segments
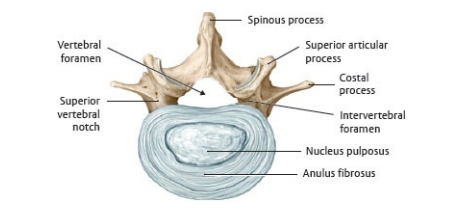
Intervertebral Disc
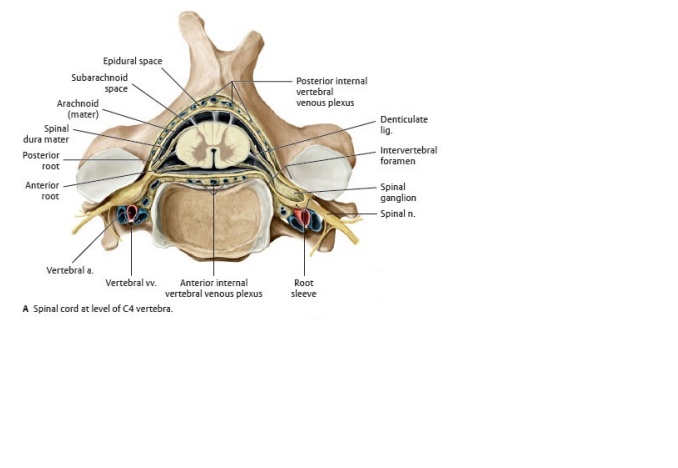
Cervical Cord (C4)
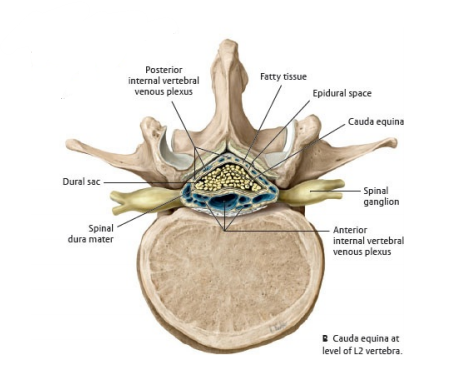
Cauda Equina (L4)
🧠 Teaching Tip: The spine is not a rigid pillar but a dynamic organ of support, protection, and motion. Each vertebra contributes to a delicate balance between stability and flexibility, while the spinal cord transforms mechanical input into neural output - the living bridge between brain and body. Understanding this integration of structure and function is the foundation of all clinical neurology and musculoskeletal medicine.
1) The vertebrae - what the bones actually look like (appearance + landmarks)
- Typical vertebra anatomy (most levels share the same “parts”):
- Vertebral body: anterior weight-bearing block (trabecular bone inside, cortical shell outside).
- Vertebral arch: pedicles (strong “pillars” from body) + laminae (roof) enclosing the vertebral foramen (spinal canal).
- Spinous process + transverse processes: levers for muscle attachment (posture and movement).
- Superior/inferior articular processes: form the facet (zygapophyseal) joints.
- Intervertebral foramina: “doorways” between adjacent pedicles where spinal nerves exit (commonly narrowed by disc bulge, osteophytes, facet hypertrophy).
- How each region looks (high-yield ID features):
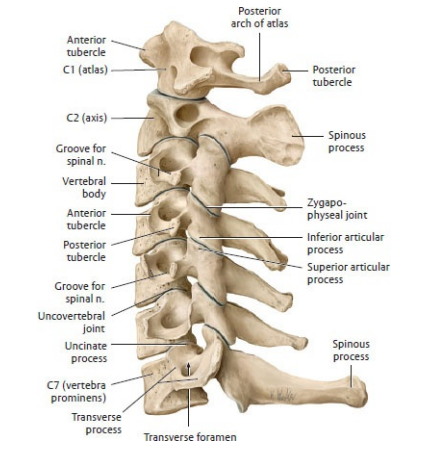
- Cervical (C3–C7): small bodies, large canal; transverse foramina in transverse processes; often bifid spinous processes (C3–C6).
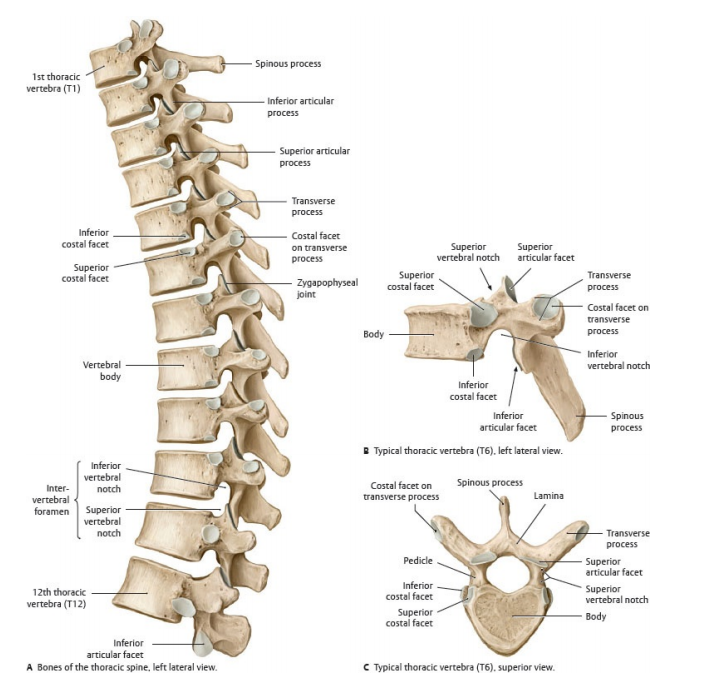
- Thoracic (T1–T12): heart-shaped bodies; long down-sloping spinous processes; costal facets on bodies/transverse processes for rib joints.
- Lumbar (L1–L5): large kidney-shaped bodies; short, thick spinous processes; robust pedicles for load; common site of degenerative stenosis.
- Sacrum: fused vertebrae; anterior/posterior sacral foramina for sacral nerves; forms the back of the pelvic ring.
- Coccyx: small fused remnants; attachment for pelvic floor ligaments and muscles.
2) The joints of the spine - where movement comes from (and where it fails)
- Intervertebral disc + vertebral bodies (a secondary cartilaginous joint / symphysis):
- Annulus fibrosus: concentric fibrocartilage lamellae resisting torsion and shear.
- Nucleus pulposus: proteoglycan-rich “gel” acting as a hydraulic shock absorber; dehydrates with age → loss of disc height and foraminal narrowing.
- Posterolateral disc herniation is common (PLL is narrower/less supportive laterally) → classic radiculopathy patterns.
- Facet (zygapophyseal) joints (true synovial joints):
- Guide and limit motion; degeneration causes local back pain, osteophytes, and contributes to foraminal stenosis.
- Orientation drives motion:
- Cervical: more horizontal/oblique → flex/extend + rotation (high mobility).
- Thoracic: more coronal + rib cage → rotation allowed, flex/extend limited.
- Lumbar: more sagittal → flex/extend favoured; rotation resisted (protects discs but stresses facets).
- Special “extra” joints:
- Uncovertebral joints (C3–C7): small lateral joints between uncinate processes and above vertebra → common source of osteophytes and cervical radiculopathy.
- Costovertebral/costotransverse joints (thoracic): rib-head and rib-tubercle articulations → explain why thoracic fractures can coexist with chest wall injury and pain.
- Sacroiliac joints: very strong synovial/anterior + syndesmotic/posterior components; limited motion but major load transfer; inflamed in spondyloarthropathies.
3) High cervical spine - C0/C1/C2 joints (appearance + function)
- Atlanto-occipital joint (C0–C1):
- Occipital condyles + superior facets of atlas → “yes” movement (flex/extend) and slight lateral flexion.
- Clinical: instability (e.g., inflammatory disease/trauma) can threaten the cervicomedullary junction.
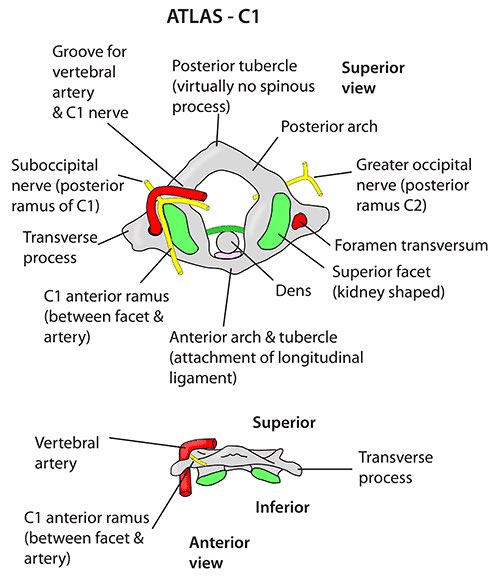
- C1 (Atlas):
- Ring-shaped; no vertebral body; large canal.
- Lateral masses bear skull weight; anterior arch has facet for the dens.
- Atlanto-axial joint (C1–C2):
- Dens (odontoid) of C2 acts as a pivot held by the transverse ligament → “no” movement (rotation).
- Clinical: dens fractures or transverse ligament disruption can cause catastrophic cord compression.
- C2 (Axis):
- Prominent dens; robust spinous process (often palpable at upper neck).
4) Spinal nerves - how bone/disc problems become neurological symptoms
- Root → nerve basics:
- Dorsal (posterior) root = sensory; contains the dorsal root ganglion (cell bodies).
- Ventral (anterior) root = motor (and preganglionic autonomics).
- They join to form a mixed spinal nerve, then split into rami to body wall/limbs.
- Numbering rule (common exam trap):
- Cervical nerves exit above their vertebrae (C5 nerve exits above C5 vertebra).
- C8 nerve exits between C7 and T1; from T1 downward, nerves exit below their vertebrae.
- Disc herniation vs which root is hit (typical pattern):
- In the lumbar spine, a posterolateral disc usually compresses the traversing root (e.g., L4/5 disc → L5 root; L5/S1 disc → S1 root).
- Foraminal stenosis more often compresses the exiting root at that level (e.g., L4 root at L4/5 foramen).
- Quick reflex/myotome anchors (useful at the bedside):
- C5–C6: biceps reflex; elbow flexion / wrist extension strength.
- C7: triceps reflex; elbow extension.
- L3–L4: knee jerk; knee extension.
- S1: ankle jerk; plantarflexion.
5) Spinal cord vs cauda equina - why the neuro signs differ
The spinal cord contains long tracts: compress it and you tend to see UMN signs below the lesion (hyperreflexia, increased tone, extensor plantar responses) once spinal shock resolves. The cauda equina is a bundle of nerve roots, so compression behaves like a multifocal radiculopathy: severe radicular pain, patchy sensory loss, LMN weakness and reduced reflexes in affected myotomes/dermatomes. The conus medullaris sits at the junction (CNS ending + sacral segments), so lesions often cause early sphincter dysfunction with mixed UMN/LMN features.
| Feature | Spinal cord lesion | Cauda equina lesion | Conus medullaris lesion |
|---|---|---|---|
| Neuro type | Often UMN below lesion | LMN (root-level) | Mixed; sacral signs prominent |
| Pain | Variable; may be less radicular | Severe radicular pain common | Variable; can be less painful |
| Saddle/perineal sensation | Depends on level | Often affected (S2–S5 roots) | Often early and prominent |
| Bladder/bowel/sexual function | May be late depending on level | Can occur; may be patchy early | Often early |
| Reflexes | Brisk below lesion (later) | Reduced/absent in affected roots | Variable |
6) Meninges & spaces - where the cord/roots sit (and why LP is safe below L2)
- Dura, arachnoid, pia surround cord and roots.
- Epidural space (outside dura): fat + venous plexus (site of epidural anaesthesia; also epidural abscess/haematoma).
- Subarachnoid space: CSF + vessels + nerve roots; below the conus it expands into the lumbar cistern containing the cauda equina.
- Lumbar puncture: usually L3/4 or L4/5, below conus to reduce cord injury risk.
- Filum terminale and denticulate ligaments help tether/stabilise the cord within the dural sac.
7) Blood supply - the vascular logic behind classic cord syndromes
- Anterior spinal artery supplies anterior ~2/3 (corticospinal + spinothalamic) → infarct causes weakness + pain/temperature loss with relatively preserved dorsal column modalities.
- Posterior spinal arteries supply dorsal columns → vibration/proprioception problems predominate.
- Segmental feeders (radicular/medullary arteries) create “watershed” vulnerability zones, especially in thoracolumbar regions.
8) UK emergency context - suspected Cauda Equina Syndrome (CES)
Suspected CES is a spinal surgical emergency. The NICE low back pain/sciatica guideline (NG59) explicitly excludes people with progressive neurological deficit or CES, emphasising that clinicians must recognise these emergencies and refer urgently. National pathways (GIRFT) centre the diagnosis on clinical features + urgent MRI, aiming for imaging “as quickly as practicably possible” to avoid permanent bladder/bowel/sexual dysfunction and lower-limb deficits.
- NICE: NG127 supports recognition/referral for suspected neurological emergencies (including CES resources).
- GIRFT pathway: provides a standardised national approach for suspected CES across settings and has been updated repeatedly (most recently into 2026).
- Practical bedside point: neurological patterning matters - LMN signs (areflexia, flaccid weakness) and saddle symptoms push you towards root/conus pathology rather than uncomplicated mechanical back pain.
References (UK + core)
- NICE NG59: Low back pain and sciatica in over 16s (excludes progressive neuro deficit / CES).
- NICE NG127: Suspected neurological conditions: recognition and referral (CES pathway resources).
- GIRFT: National Suspected Cauda Equina Syndrome (CES) Pathway (latest update set).
- RCEM: Position Statement: Cauda Equina Syndrome (ED perspective on MRI access and pathway implementation).
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery