Related Subjects:
|Atherosclerosis
|Ischaemic heart disease
|Assessing Chest Pain
|ACS - General
|ACS - STEMI
|ACS - NSTEMI
|ACS - GRACE Score
|ACS - ECG Changes
|ACS -Cardiac Troponins
|ACS - Post MI arrhythmias
|ACS: Right Ventricular Infarction
|ACS: LBBB and AMI
⚠️ Acute MI in LBBB or ventricular paced rhythm is difficult to diagnose on ECG.
LBBB causes secondary ST–T changes, so standard STEMI criteria do not apply reliably.
Use clinical judgement first: ongoing convincing ischaemic chest pain, haemodynamic instability, shock, pulmonary oedema or malignant arrhythmia should prompt urgent senior/cardiology discussion even if ECG criteria are negative.
🧠 Background
- 🫀 LBBB produces appropriate discordance: the ST segment and T wave normally point in the opposite direction to the main QRS deflection.
- 📏 The diagnostic challenge is identifying when discordance becomes excessive, suggesting acute coronary occlusion rather than normal LBBB repolarisation.
- ⚖️ Original Sgarbossa criteria are highly specific but insensitive, so they can help rule in MI but cannot safely rule it out.
- 📐 Modified Sgarbossa criteria improve sensitivity by using proportionality: ST elevation compared with the depth of the preceding S wave.
- 🧩 Barcelona criteria add further proportional and low-voltage rules, but they are less widely used and validation has been mixed.
- 🖥 Bedside echo showing a new regional wall motion abnormality can support the diagnosis, especially when ECG interpretation is difficult.
- 🩸 Serial ECGs and serial high-sensitivity troponins are useful in stable patients where the diagnosis is uncertain, but do not delay reperfusion when clinical suspicion of occlusion MI is high.
📊 ECG Criteria for Acute MI in LBBB / Paced Rhythm
| Feature |
Original Sgarbossa |
Modified Sgarbossa / Smith |
Barcelona Criteria |
| Core concept |
Absolute ST deviation rules. |
Uses proportional discordance: ST change relative to QRS size. |
Uses concordance, proportional discordance and low-voltage QRS rules. |
| Concordant ST elevation |
✅ ST elevation ≥1 mm in a lead with a positive QRS. |
✅ Same as original. |
✅ ST deviation ≥1 mm concordant with QRS polarity. |
| Concordant ST depression |
✅ ST depression ≥1 mm in V1–V3. |
✅ Same as original. |
✅ ST deviation ≥1 mm concordant with QRS polarity in any lead. |
| Discordant ST elevation |
⚠️ ST elevation ≥5 mm in a lead with negative QRS. |
📏 ST elevation ≥1 mm and ST elevation / S-wave depth ≥25%. |
📏 ST deviation ≥1 mm discordant with QRS polarity in leads where QRS voltage is ≤6 mm. |
| Accounts for QRS size? |
❌ No. |
✅ Yes - proportional rule. |
✅ Yes - includes low-voltage QRS rule. |
| Strength |
🎯 Very specific when positive. |
👍 Better balance of sensitivity and specificity. |
🔥 May improve sensitivity in some cohorts. |
| Limitation |
❌ Misses many occlusion MIs. |
🧮 Requires accurate measurement. |
🧩 Less widely taught; external validation has been variable. |
| Clinical use |
Rule-in tool. |
Commonly preferred ECG tool for suspected occlusion MI in LBBB/paced rhythm. |
Emerging/adjunctive tool; use with local expertise. |
| Image |
 |
|
|
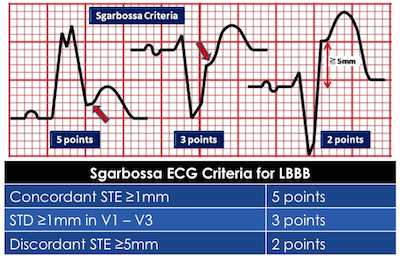
📐 Original Sgarbossa Score
| Criterion |
Points |
Meaning |
| Concordant ST elevation ≥1 mm in any lead with a positive QRS complex. |
5 |
Highly specific for acute MI. |
| Concordant ST depression ≥1 mm in V1–V3. |
3 |
Suggests posterior/anterior-septal injury pattern in LBBB. |
| Discordant ST elevation ≥5 mm in a lead with a negative QRS complex. |
2 |
Less reliable because it does not account for QRS size. |
🎯 Original Sgarbossa: a score ≥3 is traditionally considered positive.
It is useful when positive, but a negative score does not exclude acute coronary occlusion.
📏 Modified Sgarbossa / Smith Criteria
- ✅ Concordant ST elevation ≥1 mm in any lead with a positive QRS complex.
- ✅ Concordant ST depression ≥1 mm in V1–V3.
- ✅ Discordant ST elevation ≥1 mm where the ST elevation is ≥25% of the depth of the preceding S wave.
📐 Example: if the S wave is 8 mm deep, discordant ST elevation of 2 mm gives an ST/S ratio of 25%, which is concerning.
This proportional rule is the key improvement over the original fixed 5 mm rule.
🧩 Barcelona Criteria
- ✅ ST deviation ≥1 mm concordant with QRS polarity in any ECG lead.
- ✅ ST deviation ≥1 mm discordant with QRS polarity in any lead where the QRS voltage is ≤6 mm.
- 🧠 The concept is that even small ST deviation may be abnormal when the QRS complex is small.
- ⚠️ Barcelona criteria may increase sensitivity in some studies, but they are less established than Modified Sgarbossa in many emergency/cardiology settings.
🚨 Practical UK / ED Approach
- 1️⃣ Treat the patient, not the ECG: persistent ischaemic chest pain, shock, pulmonary oedema, malignant arrhythmia or haemodynamic instability needs urgent senior/cardiology review.
- 2️⃣ Get old ECGs: determine whether LBBB is new, old, or paced rhythm; new LBBB alone is not automatically STEMI.
- 3️⃣ Apply Modified Sgarbossa: any positive criterion in the right clinical context should prompt urgent cardiology/cath-lab discussion.
- 4️⃣ Repeat ECGs: dynamic changes increase concern even if initial criteria are negative.
- 5️⃣ Use bedside echo: new regional wall motion abnormality supports acute coronary occlusion.
- 6️⃣ Use troponin intelligently: do not wait for troponin if the patient is unstable or the story strongly suggests occlusion MI; in stable uncertainty, serial high-sensitivity troponin and delta change are useful.
- 7️⃣ Discuss early: if in doubt, speak to interventional cardiology rather than waiting for criteria to become obvious.
⚠️ When to Activate / Discuss Cath Lab Urgently
- Ongoing convincing ischaemic symptoms with any positive Sgarbossa or Modified Sgarbossa feature.
- Ongoing chest pain with haemodynamic instability, cardiogenic shock or acute pulmonary oedema.
- Recurrent malignant ventricular arrhythmia.
- New regional wall motion abnormality on echo with compatible symptoms.
- Dynamic ECG change or rising clinical concern despite non-diagnostic ECG.
- Persistent symptoms in a high-risk patient where LBBB/paced rhythm makes ECG interpretation unreliable.
🚫 Common Pitfalls
- ❌ Assuming new LBBB alone equals STEMI.
- ❌ Reassuring yourself because Sgarbossa is negative.
- ❌ Waiting for troponin in an unstable patient with ongoing ischaemic symptoms.
- ❌ Ignoring proportionality: 3 mm ST elevation may be very abnormal if the S wave is only 6 mm deep.
- ❌ Forgetting posterior MI, which may be electrically hidden in LBBB.
- ❌ Not comparing with previous ECGs.
📝 Exam Pearls
- 🫀 LBBB causes appropriate discordance: ST/T usually point opposite to the QRS.
- 🚨 Concordant ST elevation in LBBB is never reassuring.
- 📏 Modified Sgarbossa replaces the old “5 mm discordant STE” rule with a proportional rule.
- 🎯 Original Sgarbossa is specific but insensitive: positive helps rule in, negative does not rule out.
- 🩸 Troponin supports the diagnosis, but persistent ischaemic symptoms and instability should drive urgent action.
- 🖥 Echo can help when ECG is obscured by LBBB or pacing.
🧠 Teaching Note
In LBBB, the ventricles activate abnormally, so repolarisation is abnormal too.
That is why ST elevation in the opposite direction to a deep S wave can be normal “appropriate discordance”.
The clever part of Modified Sgarbossa is proportionality: a large QRS can tolerate more discordant ST shift, while a small QRS cannot.
Clinically, however, no algorithm replaces the story - prolonged crushing chest pain with instability deserves urgent cardiology discussion even when the ECG is hard to interpret.
📚 References
