
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Epidural Spinal abscess
Related Subjects: |Transverse myelitis |Acute Disseminated Encephalomyelitis |Cervical spondylosis |Spinal Cord Anatomy |Acute Disc Prolapse |Spinal Cord Compression |Spinal Cord Haematoma |Foix-Alajouanine syndrome |Cauda Equina |Conus Medullaris syndrome |Anterior Spinal Cord syndrome |Central Spinal Cord syndrome |Brown-Sequard Spinal Cord syndrome
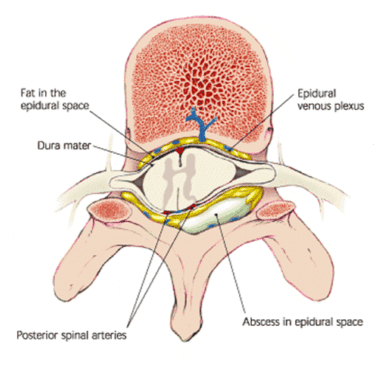
🧠 A spinal epidural abscess (SEA) is a rare but life-threatening infection in the epidural space, between vertebrae and dura mater. ⚡ It can rapidly compress the spinal cord → causing severe neurological deficits, paralysis, or death if untreated.
📖 About
- 🔴 Presents with severe back pain ± progressive weakness in legs/arms over hours–days.
- 🦠 Staphylococcus aureus (incl. MRSA) = most common pathogen.
- 🩸 Infection usually spreads haematogenously; may also extend from nearby bone/soft tissue or follow surgery.
- ⚠️ Classical triad = back pain + fever + neurological deficit (but only present in 10–15% at diagnosis).
🔬 Aetiology
- Haematogenous spread: Skin infection, UTI, endocarditis.
- Direct extension: Vertebral osteomyelitis, psoas abscess.
- Post-procedure: Spinal surgery, epidural catheterisation, nerve blocks.
- Trauma: Penetrating injury or open wound.
⚡ Risk Factors
- Diabetes mellitus.
- IV drug use 💉.
- Immunosuppression (HIV, steroids, chemo, transplant).
- Chronic kidney disease, alcoholism.
- Recent spinal surgery or invasive spinal procedure.
🩺 Clinical Presentation
- 🌡 Severe localised back pain, spinal tenderness.
- 🤒 Fever, malaise, sepsis signs.
- ⚡ Progressive motor/sensory deficits → paraparesis, quadriparesis, sensory level.
- 🚽 Autonomic dysfunction: bladder/bowel disturbance.
🚨 Red Flags
- Rapidly worsening weakness or paralysis.
- High fever, septic shock features.
- Recent spinal surgery or procedure.
- History of IV drug use or immunosuppression.
🧪 Investigations
- 🖥 MRI spine with contrast: Gold standard - defines abscess extent, cord compression.
- 🧬 Blood cultures: Often positive for S. aureus.
- 📊 Bloods: Raised CRP, ESR, WCC (inflammatory response).
- 🩻 CT spine: Alternative if MRI contraindicated (less sensitive for soft tissue).
🚨 SEA is a neurosurgical emergency. Delay in diagnosis/treatment greatly increases risk of permanent paralysis or death.
💊 Management
- Empirical IV Antibiotics: Start broad-spectrum (incl. MRSA cover e.g., vancomycin + ceftriaxone) → refine once cultures available. ⚠️ In unstable septic patients → do not delay antibiotics for imaging.
- Surgical Drainage: Laminectomy or CT-guided aspiration to relieve compression & obtain cultures.
- Supportive Care: Pain relief, neuro monitoring, bladder/bowel care, VTE prophylaxis, rehab for residual deficits.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery