
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Central and Branch Retinal Vein Occlusion (CRVO/BRVO)
⚠️ Central Retinal Vein Occlusion (CRVO) is an ophthalmic emergency. 👁️ Patients must be urgently reviewed by ophthalmology to exclude other acute causes of visual loss and to guide management. Visual prognosis depends on the degree of ischaemia and complications such as macular oedema and neovascularisation.
ℹ️ About
- Venous outflow obstruction of the central retinal vein → retinal ischaemia & oedema.
- May occur due to thrombophilia or compression by adjacent arteriosclerotic artery.
- Common cause of painless monocular visual loss in older adults.
🧬 Aetiology
- Compression of vein by arteriosclerotic central retinal artery (shared adventitia at lamina cribrosa).
- Thrombus formation → stagnation of blood flow, venous congestion, ischaemia.
- Visual loss due to macular oedema or retinal neovascularisation.
Risk Factors (Arteriosclerotic & Haematological)
- 🩸 Hypertension, diabetes, hyperlipidaemia.
- 🚬 Smoking.
- 👁️ Glaucoma (raised intraocular pressure).
- 🧪 Hyperviscosity states: polycythaemia, multiple myeloma, Waldenström’s macroglobulinaemia, leukaemia.
- 💉 Thrombophilia, esp. in patients <50 yrs.
- Inflammatory eye disease (rare).
🩺 Clinical Features
- ⚡ Painless monocular loss of vision (may be sudden or progressive).
- Fundus findings:
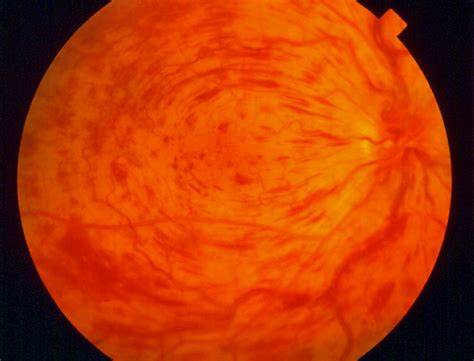
- “Blood and thunder” appearance → widespread flame-shaped haemorrhages.
- Cotton wool spots, dilated & tortuous veins.
- Macular oedema, swollen optic disc.
- History: ask about vascular risk factors, malignancy, personal/family history of DVT/PE.
CRVO
Florid Haemorrhages and Dilated Veins
BRVO
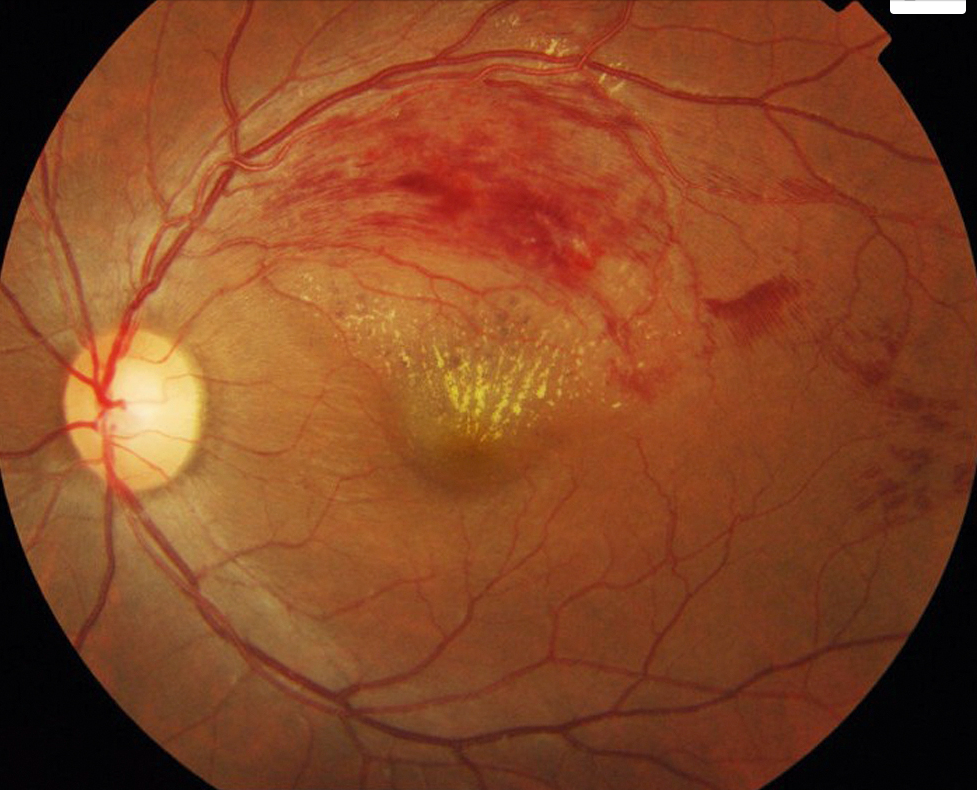
Differential Diagnosis
- Central retinal artery occlusion (CRAO).
- Retinal detachment.
- Migrainous aura with transient visual loss.
- Optic neuritis (esp. if painful visual loss).
🔎 Investigations
- 🧪 Bloods: FBC, ESR, U&E, glucose, lipid profile.
- ECG ± echocardiogram if cardiac risk factors.
- Thrombophilia screen if age <50 or no risk factors.
- OCT (optical coherence tomography) to assess macular oedema.
- Fluorescein angiography (ophthalmology) to grade ischaemic vs non-ischaemic CRVO.
💊 Management
- 📉 Risk factor optimisation: treat hypertension, diabetes, lipids; smoking cessation.
- 💊 Consider low-dose Aspirin (75 mg OD) for vascular risk reduction.
- 👁️ Ophthalmology-directed:
- Intravitreal anti-VEGF (e.g. ranibizumab, aflibercept) for macular oedema.
- Intravitreal corticosteroids (e.g. dexamethasone implant) if VEGF unsuitable.
- Laser photocoagulation if neovascularisation develops (to reduce risk of neovascular glaucoma).
- 🔎 Monitor for complications: rubeotic/neovascular glaucoma, vitreous haemorrhage, retinal detachment.
References
🧾 Clinical Case 1 – CRVO (Ischaemic Type)
A 72-year-old man with poorly controlled hypertension and type 2 diabetes presents with sudden painless loss of vision in his left eye. Fundoscopy shows a classic "blood and thunder" appearance with widespread retinal haemorrhages, cotton-wool spots, and optic disc swelling. 👉 Diagnosis: Ischaemic CRVO. 👉 Management: urgent referral to ophthalmology for anti-VEGF therapy, pan-retinal photocoagulation if neovascularisation, and systemic risk factor control.
🧾 Clinical Case 2 – CRVO (Non-Ischaemic Type)
A 60-year-old woman with a history of glaucoma and hyperlipidaemia complains of blurred vision and floaters in her right eye, but no complete visual loss. Fundoscopy reveals venous engorgement, scattered retinal haemorrhages, and macular oedema. 👉 Diagnosis: Non-ischaemic CRVO. 👉 Management: anti-VEGF injections for macular oedema, regular monitoring for progression to ischaemic CRVO, and treatment of underlying glaucoma and dyslipidaemia.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery