
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Anatomy and Phsyiology of the Ear
📚 Related Subjects: |AP of the Oesophagus |AP of the Diaphragm |AP of the Large Bowel (Colon, Rectum, Anal Canal) |AP of Small Bowel |AP of the Biliary system |AP of the Bone Marrow |AP of the Eye |AP of the Pharynx |AP of the Larynx |AP of the Ear |AP of the Nose |AP of Male Genitalia |AP of the Breast |AP of the Stomach |AP of the Rectum |AP of the Spleen
The ear is a specialised sensory organ responsible for hearing 🎧 and balance ⚖️. It works by (1) capturing and directing sound (external ear), (2) amplifying and transmitting vibration (middle ear), and (3) converting mechanical energy into neural signals (inner ear/cochlea). Balance depends on the vestibular labyrinth, which detects head motion and position and drives reflexes that stabilise vision (VOR) and posture.
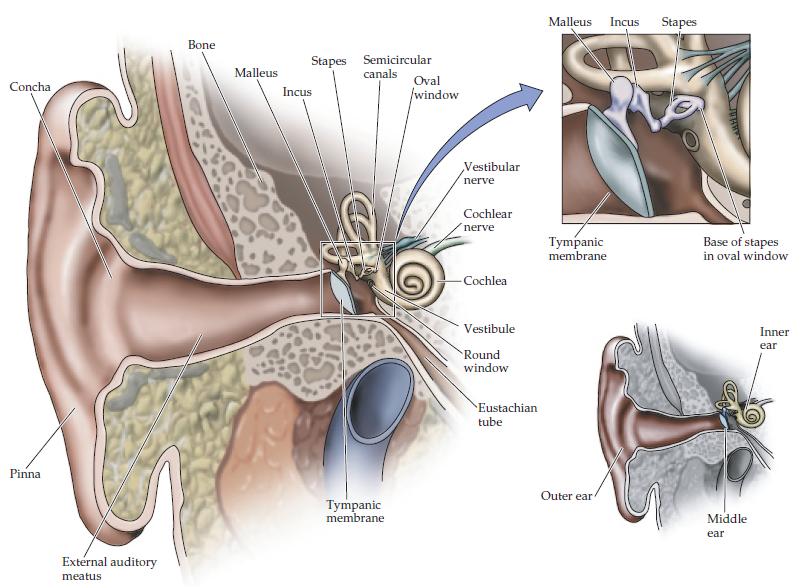
1) External Ear (Sound Collection & Protection) 🌬️
The external ear “funnels” sound into the canal, with subtle pinna shape cues helping localisation (especially vertical localisation). The ear canal also protects the tympanic membrane and maintains a hostile environment for pathogens via cerumen (earwax).
🏷️ A) Auricle (Pinna)
- Structure: elastic cartilage covered by thin skin (lobule is fatty, no cartilage).
- Key landmarks: helix, antihelix, tragus, antitragus, concha, lobule.
- Function: collects sound; assists sound localisation by altering frequency spectra before sound enters canal.
- Clinical: auricular haematoma (often wrestling/boxing) can disrupt cartilage blood supply → “cauliflower ear” if not drained.
🌀 B) External Auditory Canal
- Length: ~2.5 cm; lateral third cartilaginous, medial two-thirds bony.
- Lining: skin with hair follicles (outer canal) + ceruminous glands producing cerumen.
- Cerumen roles: hydrophobic barrier, traps debris, mildly acidic and antimicrobial.
- Clinical: otitis externa causes canal pain and tenderness (classically pain on tragal pressure or pinna movement).
🥁 C) Tympanic Membrane (Eardrum)
- Structure: thin conical membrane; pars tensa (main vibrating portion) and pars flaccida.
- Function: converts airborne sound waves into mechanical vibration of ossicles.
- Clinical: perforation → conductive hearing loss; retraction pockets (esp pars flaccida) may progress to cholesteatoma.
2) Middle Ear (Impedance Matching & Amplification) 🔧
The middle ear is an air-filled amplifier. Its core job is impedance matching: efficiently transferring sound from air (low impedance) to cochlear fluid (high impedance). Without the ossicles, most sound would reflect at the air–fluid boundary and hearing would be dramatically reduced.
🏛️ A) Middle Ear Cavity
- Location: within the temporal bone (tympanic cavity).
- Contents: ossicles, muscles, nerves, air mucosa.
- Windows:
- Oval window: stapes footplate transmits vibration into inner ear.
- Round window: pressure release membrane allowing cochlear fluid displacement.
🦴 B) Ossicles (Malleus, Incus, Stapes)
- Malleus (“hammer”) attached to tympanic membrane (manubrium).
- Incus (“anvil”) bridges malleus and stapes.
- Stapes (“stirrup”) attaches to oval window.
- Amplification mechanisms:
- Area ratio: large tympanic membrane area → small stapes footplate → increases pressure at oval window.
- Lever action: ossicular chain acts as a lever to increase force transmission.
- Clinical: otosclerosis (stapes fixation) → progressive conductive hearing loss; may show Carhart notch on audiogram.
💪 C) Middle Ear Muscles (Protective Reflex)
- Stapedius (CN VII) reduces stapes movement.
- Tensor tympani (CN V3) tenses tympanic membrane.
- Acoustic reflex: contraction in response to loud sound, protecting cochlea (limited effectiveness for sudden impulse noise).
- Clinical: facial nerve palsy may cause hyperacusis (stapedius weakness).
🌬️ D) Eustachian (Auditory) Tube
- Connection: middle ear ↔ nasopharynx.
- Functions: equalises pressure; drains secretions; ventilates middle ear.
- Opens during: swallowing, yawning (tensor veli palatini activity).
- Clinical: dysfunction after URTI/allergy → negative middle ear pressure and effusion (“glue ear”); children are predisposed due to shorter, more horizontal tube.
3) Inner Ear (Labyrinth): Hearing + Balance 🧠
The inner ear is a fluid-filled sensory transducer. It contains the cochlea (hearing) and the vestibular apparatus (balance). Mechanical movement of endolymph/perilymph deflects hair cell stereocilia, converting motion into graded receptor potentials and then action potentials in CN VIII.
🌀 A) Cochlea (Hearing)
- Structure: spiral bony labyrinth (≈2.5 turns) surrounding the modiolus.
- Three chambers:
- Scala vestibuli (perilymph) begins at oval window.
- Scala media / cochlear duct (endolymph) contains organ of Corti.
- Scala tympani (perilymph) ends at round window.
- Key membranes: Reissner’s membrane (vestibuli–media), basilar membrane (media–tympani).
- Organ of Corti: sensory hair cells + supporting cells on basilar membrane.
- Tonotopy:
- Base: high frequency (stiff, narrow basilar membrane).
- Apex: low frequency (floppier, wider basilar membrane).
- Clinical: noise-induced hearing loss often affects high frequencies first (basal cochlea vulnerability).
⚡ Cochlear Transduction (How sound becomes nerve impulses)
Hair cells sit in a potassium-rich endolymph environment. Deflection of stereocilia opens mechanically gated channels, allowing K+ influx from endolymph (unusual vs most neurons), depolarising the hair cell and triggering neurotransmitter release onto auditory nerve fibres.
- Step 1: stapes pushes oval window → perilymph wave propagates.
- Step 2: basilar membrane vibrates at a frequency-specific point.
- Step 3: stereocilia shear against the tectorial membrane → ion channels open.
- Step 4: hair cell depolarises → Ca2+ entry → glutamate release → CN VIII firing.
- Outer hair cells: act as an active amplifier (electromotility) sharpening tuning and improving sensitivity.
- Clinical: aminoglycosides and loop diuretics can be ototoxic; damage may be cochlear (hearing) and/or vestibular (balance).
⚖️ B) Vestibular System (Balance)
- Semicircular canals (3 canals) detect angular acceleration (head rotation).
- Each canal has an ampulla containing the crista ampullaris and cupula.
- Endolymph inertia bends the cupula → deflects hair cells → signals rotation direction/speed.
- Otolith organs: utricle and saccule detect linear acceleration and gravity.
- Macula hair cells are topped by otoconia (calcium carbonate crystals).
- Movement shifts otoconia → bends stereocilia.
- Clinical: BPPV occurs when otoconia dislodge (often into posterior canal) → brief positional vertigo; treated with canalith repositioning (Epley manoeuvre).
👁️ Vestibulo-ocular reflex (VOR)
- Purpose: stabilises gaze during head movement (keeps vision steady).
- Mechanism: head turns right → right vestibular firing increases → eyes reflexively move left.
- Clinical: abnormal head impulse test suggests peripheral vestibular dysfunction.
4) Nerve Supply (High-yield) 🧠
- CN VIII (Vestibulocochlear):
- Cochlear division: hearing.
- Vestibular division: balance.
- CN VII (Facial): passes through middle ear region; supplies stapedius; gives chorda tympani (taste anterior 2/3 tongue).
- CN IX (Glossopharyngeal): sensory to middle ear mucosa and Eustachian tube.
- CN V (Trigeminal): contributes sensation (external ear/canal regions).
- Clinical: vestibular schwannoma (acoustic neuroma) → unilateral SNHL, tinnitus, imbalance; may affect CN VII as it enlarges.
5) Vascular Supply 🫀
- External ear: superficial temporal and posterior auricular arteries.
- Middle ear: multiple small branches (including anterior tympanic from maxillary; ascending pharyngeal contributions).
- Inner ear: labyrinthine artery (often from AICA or basilar) - an end-artery type supply.
Clinical: vascular compromise can cause sudden sensorineural hearing loss and/or acute vestibular symptoms.
6) Physiology of Hearing (From Sound Wave to Cortex) 🎶
Sound is a pressure wave. The external ear directs it to the tympanic membrane, the middle ear amplifies it, and the cochlea converts it into neural firing patterns. The brain then extracts pitch (frequency), loudness (amplitude), and location (timing and intensity differences between ears).
- Conductive pathway: pinna → canal → tympanic membrane → ossicles → oval window.
- Sensorineural pathway: cochlea hair cell transduction → cochlear nerve → brainstem nuclei → inferior colliculus → medial geniculate body → auditory cortex.
- Sound localisation:
- Interaural time difference (low-frequency localisation).
- Interaural intensity difference (high-frequency “head shadow” effect).
7) Clinical Integration (Quick but High Yield) ⚕️
- Conductive hearing loss: external/middle ear problem (wax, otitis media, perforation, ossicular disease).
📌 Rinne/Weber helps bedside differentiation. - Sensorineural hearing loss: inner ear/CN VIII/central pathway problem (noise, presbycusis, ototoxicity, sudden SNHL).
- Otitis media: Eustachian tube dysfunction → effusion/infection; mastoiditis is a serious complication.
- Cholesteatoma: keratinising epithelium growth with erosion risk (ossicles) → conductive loss; may cause chronic discharge.
- Vertigo differentials: BPPV (seconds, positional), vestibular neuritis (days, severe), Ménière’s (episodic vertigo + tinnitus + aural fullness + fluctuating hearing loss).
✅ Summary
The ear has three parts: external (sound capture), middle (impedance matching via ossicles and pressure equalisation via Eustachian tube), and inner (cochlea for hearing and vestibular labyrinth for balance). Cochlear hair cells convert basilar membrane vibration into neural firing using a unique K+-rich endolymph system, while vestibular organs detect rotation (semicircular canals) and linear acceleration (utricle/saccule) and stabilise gaze via the VOR. Clinical patterns (conductive vs sensorineural hearing loss; positional vs persistent vertigo) map directly onto this anatomy.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery