Related Subjects:
|Assessing Coma and Management
|Glasgow Coma scale
|Acute Poisoning
|Trauma: Traumatic Brain Head Injury (TBI)
|Acute Anaphylaxis
|Basic Life Support
|Advanced Life Support
|Acute Stroke Assessment
|Brain Herniation syndromes
|Haemorrhagic stroke
|Acutely ill patient
|Distributive Shock
|Hypovolaemic or Haemorrhagic Shock
|Obstructive Shock
|Septic Shock and Sepsis
|Shock (General Assessment)
🧠 Coma Management Guide
⚠️ If the cause of coma is uncertain (e.g. CT negative), always consider giving the CAND bundle:
💉 Cefotaxime (meningitis cover),
💊 Aciclovir (HSV encephalitis),
💉 Naloxone (opiates),
🍬 Dextrose ± Pabrinex (thiamine, prevent Wernicke’s).
This covers the major reversible causes until further information is available.
| 🛠️ Coma Management Overview |
- 🔄 Initial assessment: ABC, high-flow O₂, recovery position. If GCS < 9, seek anaesthetic review and prepare for intubation.
- 🖥️ Early CT head (and C-spine if trauma). Exclude SDH, EDH, ICH, tumour.
- 🧠 If CT shows bleed or mass → urgent neurosurgery referral.
- 🧩 If CT is normal → think metabolic, infective, toxic, endocrine causes:
- 💊 Opiates: Pinpoint pupils, low GCS → IV Naloxone 0.4 mg, repeat to max 2 mg.
- 🍬 Hypoglycaemia: IM Glucagon 1 mg and/or IV Dextrose (200 ml 10-20% or 50 ml 50%).
- 🦠 Meningitis: IV Cefotaxime immediately.
- 🧬 HSV encephalitis: IV Aciclovir 10 mg/kg q8h.
- 🧪 Endocrine: Suspected Addisonian crisis → Hydrocortisone 100 mg IV stat.
- 🌡️ Thyroid crisis: Consider IV T3/T4 for myxoedema coma (bradycardia, hypothermia).
- 🧲 Seizure (Convulsive and non convulsive): Lorazepam 2-4 mg IV, see Status, EEG if uncertain.
- 🦟 Cerebral malaria: Travel history? → IV Quinine, blood films.
- ⬆️ Raised ICP and coning:
- Intubate + hyperventilate (target pCO₂ 28–32 mmHg).
- IV Mannitol boluses if appropriate.
- Definitive neurosurgery (EVD, decompression, clot evacuation).
|
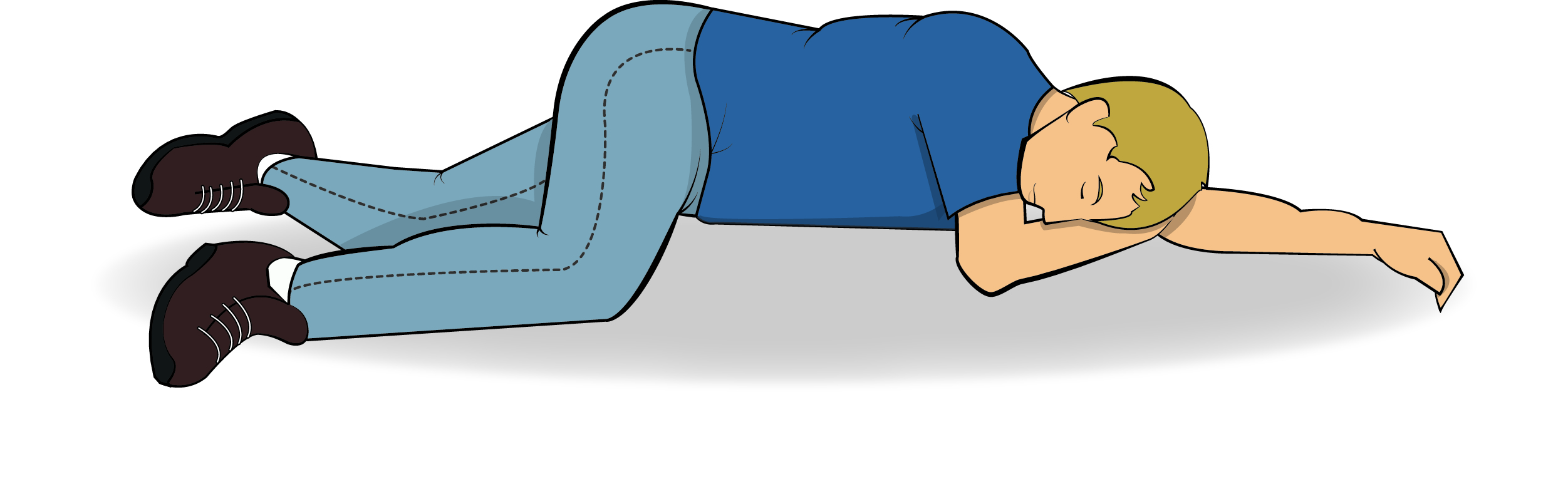
🛌 Recovery Position
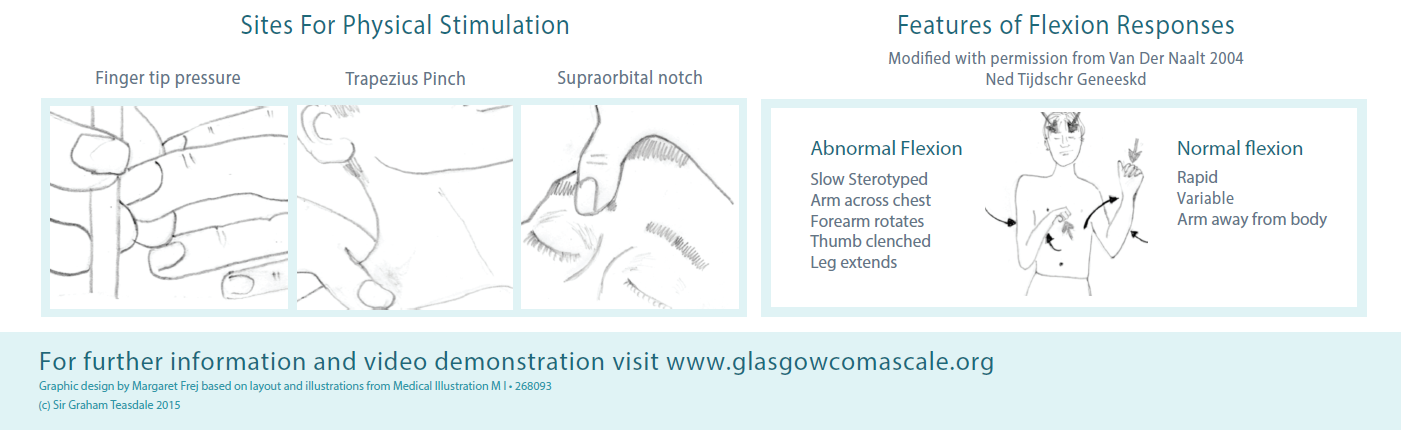
📏 Assessment of Coma: GCS & Pupils
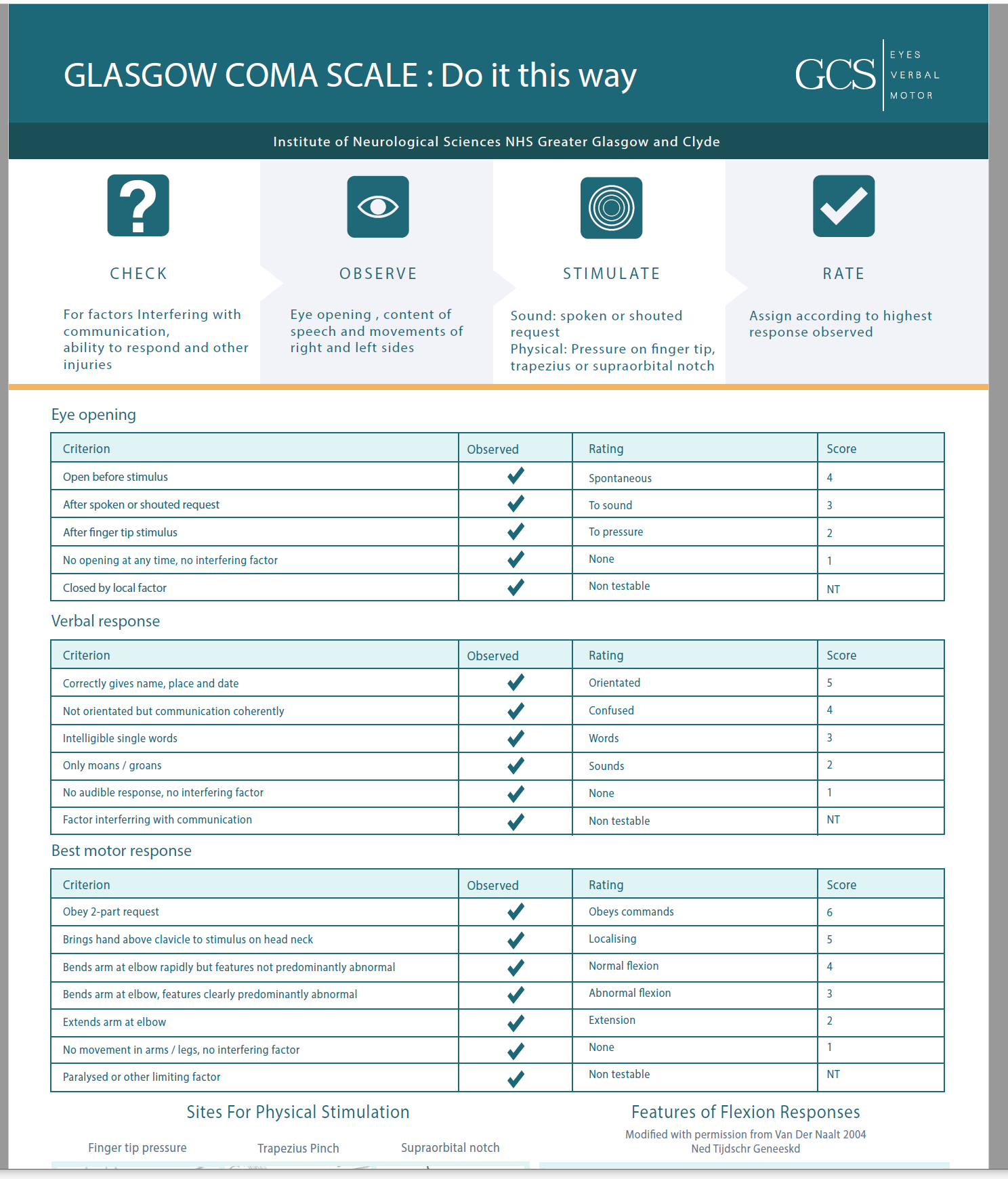
📄 Download GCS Chart
🧠 Pathophysiology of Coma (ARAS)
- Consciousness requires intact Ascending Reticular Activating System (ARAS) + cortex.
- ARAS = brainstem nuclei → thalamus → cortex.
- Coma occurs with ↑ ICP, bilateral cortical/thalamic damage, or brainstem dysfunction.
- Pupils give localising clues:
🔴 Bilateral dilated, fixed → herniation/brainstem failure.
🔵 Pinpoint → pons or opioids.
⚖️ Unequal → structural lesion compressing CN III.
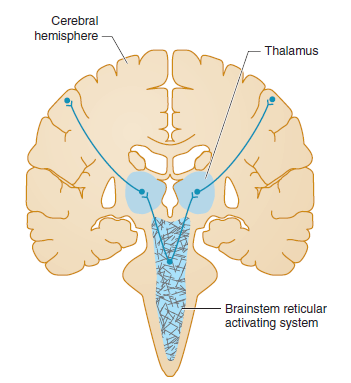
🧩 Consciousness depends on ARAS (midbrain/pons) + both cerebral hemispheres.
Structural lesions or diffuse metabolic insults can both produce coma.
🧪 Differential Diagnosis: CT & Glucose First
| Cause | Clues | Management |
|---|
| 🍬 Hypoglycaemia | Low CBG | IV Dextrose |
| 💊 Opiate toxicity | Pinpoint pupils | IV Naloxone |
| 🧠 Stroke | Focal neurology | CT head, stroke pathway |
| ⚡ Post-ictal | History of seizure | Recovery position, treat status |
| 🦠 Meningitis/Encephalitis | Fever, neck stiffness | Cefotaxime + Aciclovir |
| ☠️ CO poisoning | Exposure, headache, cherry-red skin | 100% O₂ ± hyperbaric |
| 🤕 Head injury | History of trauma | CT head/C-spine |
| 💧 Hyponatraemia | Na <115, seizures | Hypertonic saline |
| 🧬 Sepsis | Fever, shock | IV Tazocin + Gentamicin |
| 📟 NCSE | Unresponsive, subtle eye movements | EEG, Lorazepam |
| 💥 SDH/EDH | Head trauma | Neurosurgery + Mannitol |
| 🦟 Cerebral malaria | Travel history | IV Quinine |
⚡ Pupils in Coma
| Pupil Type | Description | Causes |
|---|
| Normal | 3–4 mm, reactive | Metabolic causes |
| Thalamic | ~2 mm, reactive | Thalamic compression |
| Fixed dilated | >7 mm, unreactive | Herniation, CN III compression |
| Midsized fixed | ~5 mm, unreactive | Midbrain lesion |
| Pinpoint | 1–1.5 mm, minimal reaction | Pons, opioids, organophosphates |
| Asymmetric | Anisocoria | Structural lesion, CN III palsy |
🚨 Signs of Trauma
- 🐼 Raccoon eyes (periorbital bruising).
- 🎧 Battle’s sign (mastoid bruising).
- 🩸 Haemotympanum.
- 💧 CSF rhinorrhoea/otorrhoea (confirm with β-2 transferrin).
- 👆 Palpable depressed skull fracture.
📊 Pathophysiologic Patterns
| Feature | Supratentorial | Subtentorial | Diffuse/Metabolic |
|---|
| Pupils | Normal or dilated with herniation | Midsized (midbrain), pinpoint (pons) | Normal/reactive; pinpoint (opiates); dilated (anticholinergics) |
| Eye movements | May show gaze preference | Abnormal adduction/abduction | Usually preserved unless sedated |
| Motor | Often asymmetric | Asymmetric (uni) or symmetric (bi) | Usually symmetric |
📚 Teaching Commentary
Coma is a syndrome, not a diagnosis. Always think structural vs metabolic.
🔍 Pupils are the fastest localising sign: normal = metabolic, abnormal = structural.
🇬🇧 In UK practice, juniors should remember:
“CAND for coma if CT is normal” → Cefotaxime, Aciclovir, Naloxone, Dextrose + Pabrinex.
This covers the major reversible killers until more is known.
GCS < 8 = intubate. Always immobilise the neck if trauma suspected.
References
