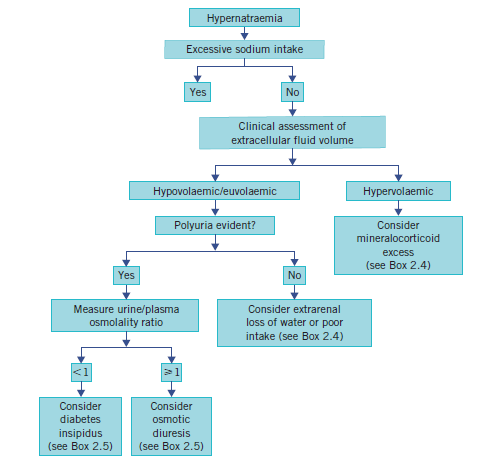
Hypernatraemia
Related Subjects:
| Sodium Physiology
| Hyponatraemia
| TURP Hyponatraemia syndrome
| Hypernatraemia
| Diabetes Insipidus
⚠️ Hypernatraemia is almost always due to water loss rather than sodium gain.
It carries a high mortality (>50% if severe).
⚖️ Key principle: Correct sodium slowly (≤10–12 mmol/L/day) to avoid cerebral oedema.
| 💧 Management Summary – Guided by Clinical Assessment of Dehydration |
- 🧪 Hypernatraemia: Avoid rapid correction; monitor I/O and use NEWS for deterioration.
- 🟢 Mild–Moderate (Na 146–155): Encourage oral fluids if able; otherwise IV fluids.
- 🔴 Moderate–Severe (>155): IV 5% Dextrose or 0.45% Saline (often 3–6 L over 24h).
- ⚕️ Underlying cause: Free water loss most common → replace orally if possible; IV if not.
- 🔍 Identify contributors: Hyperglycaemia, hypercalcaemia, hypokalaemia, DI, fever, poor oral intake.
|
📖 About
- Usually reflects free water loss, not sodium excess.
- Older adults at risk due to blunted thirst and impaired access to fluids.
- Severe hypernatraemia → mortality >50%.
🧬 Aetiology & Pathophysiology
- ↑ Serum osmolality draws water out of cells → cellular shrinkage.
- Cells adapt after ~24h by producing osmolytes to retain water.
- Normal response: osmoreceptors trigger thirst + ADH release (vasopressin).
- Hypernatraemia develops when water intake is impaired.
📌 Causes
- Water Loss:
- GI: severe vomiting/diarrhoea
- Skin/lungs: burns, sweating, fever, hyperventilation
- Renal: osmotic diuresis (hyperglycaemia, mannitol), post-obstructive polyuria
- ADH Deficiency/Resistance: Cranial DI (head trauma, pituitary surgery), nephrogenic DI (e.g. lithium).
- Iatrogenic: Hypertonic IV solutions, sodium bicarbonate, salt tablets.
- Endocrine: Rare – Conn’s syndrome, ectopic ACTH.
🩺 Clinical Presentation
- Early: intense thirst, dehydration, lethargy.
- Neuro: confusion, delirium, coma, seizures.
- Polyuria: suggests DM (check CBG) or DI.
- Severe brain shrinkage → risk of subdural haemorrhage (bridging vein rupture).
- Thrombosis risk ↑ with circulatory concentration.
🔬 Investigations
- FBC, U&E, calcium, potassium, glucose, CRP.
- Serum & urine osmolality, urine sodium.
- Lithium levels (if on lithium).
- Neuroimaging (CT/MRI) if cranial DI suspected.
⚠️ Complications
- Intracranial haemorrhage (subarachnoid, subdural) due to vascular stretch/rupture.
- Cerebral oedema if sodium is corrected too rapidly.
- Seizures, coma, death.
🧮 Calculating Water Deficit
- Total Body Water (TBW): Weight (kg) × 0.6 (men) or 0.5 (women).
- Deficit (L): TBW × ((Serum Na / 140) − 1).
- Replace over 2–3 days to avoid rapid shifts.
💊 Management
- Cautious Rehydration: 0.45% NaCl or 5% Dextrose; aim ≤10 mmol/L correction in 24h.
- If hypovolaemic shock: Resuscitate first with isotonic saline (0.9% NaCl), then switch to hypotonic fluids.
- Check and stop diuretics; correct electrolytes (Ca, K, glucose).
- Cranial DI: DDAVP (desmopressin).
- Nephrogenic DI: Stop lithium; give amiloride 2.5–10 mg/day; NSAIDs may help.
- Frequent monitoring: Sodium every 4–6 hours, daily weights, strict fluid balance.
✅ Key Pearls
- 🚰 Encourage oral water intake if safe.
- ⚠️ Rapid correction = risk of cerebral oedema → seizures, herniation.
- 🔄 Always treat underlying cause (infection, hyperglycaemia, DI, iatrogenic fluids).
