Hydrocephalus and Stroke
Related Subjects:
|Acute Stroke Assessment (ROSIER&NIHSS)
|Atrial Fibrillation
|Atrial Myxoma
|Causes of Stroke
|Ischaemic Stroke
|Cancer and Stroke
|Cardioembolic stroke
|CT Basics for Stroke
|Endocarditis and Stroke
|Haemorrhagic Stroke
|Stroke Thrombolysis
|Hyperacute Stroke Care
🧠 Introduction
- This section covers acquired hydrocephalus caused by impaired CSF flow/absorption after stroke (not congenital/childhood hydrocephalus).
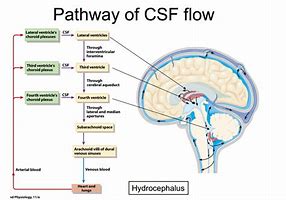
💧 Cerebrospinal Fluid (CSF) Physiology
- CSF is mainly produced by the choroid plexuses: lateral ventricles (~70%), third ventricle (~5%), fourth ventricle (~5%); plus ependymal cells (~20%).
- Flows: lateral ventricles ➝ foramen of Monro ➝ third ventricle ➝ aqueduct of Sylvius (narrow, ~2 mm ➝ common blockage site) ➝ fourth ventricle ➝ foramina of Luschka & Magendie ➝ subarachnoid space.
- Absorbed via arachnoid villi into venous sinuses.
- Blockage above villi ➝ non-communicating hydrocephalus.
Blockage at villi ➝ communicating hydrocephalus.
- Production driven by Na⁺/K⁺ ATPase (Na⁺ secretion draws water). Daily ~500 mL produced; circulating volume 100–150 mL ➝ replaced 3× daily.
- Functions: cushions brain (reduces effective weight 1400 g → 50 g), clears waste, maintains ventricular/subarachnoid homeostasis.
- ⚠️ Acute untreated hydrocephalus is fatal - enough CSF is made in 3 days to fill skull volume.
📌 Types of Hydrocephalus
- Communicating: Ventricles remain connected with subarachnoid space but absorption impaired.
- Non-communicating: Blockage prevents ventricular–subarachnoid communication (common in stroke ➝ aqueduct or 4th ventricle obstruction).
- Obstructive hydrocephalus after stroke ➝ swelling obstructs aqueduct/fourth ventricle ➝ ↑ ICP and brainstem herniation risk.
- ⏱️ Up to 20% of SAH patients develop hydrocephalus within 3–5 days, especially with intraventricular blood.
🩺 Clinical Presentation
- Headache, nausea, vomiting 🤢
- Dyspraxia, seizures ⚡
- Eye signs: impaired gaze, papilloedema 👀
- Drowsiness ➝ coma ➝ death if untreated 🛑
🚧 Common Sites of CSF Flow Obstruction
- 🔸 Foramen of Monro: Rare; tumours, blood, oedema, or colloid cysts can block one/both foramina.
- 🔸 Aqueduct of Sylvius: Commonest site; congenital/acquired stenosis, tumour, or blood ➝ ventriculomegaly upstream.
- 🔸 Outlet foramina of 4th ventricle (Luschka, Magendie): Blocked by posterior fossa tumour, blood, oedema, or post-infective scarring ➝ failure of CSF exit.
🔎 Investigations
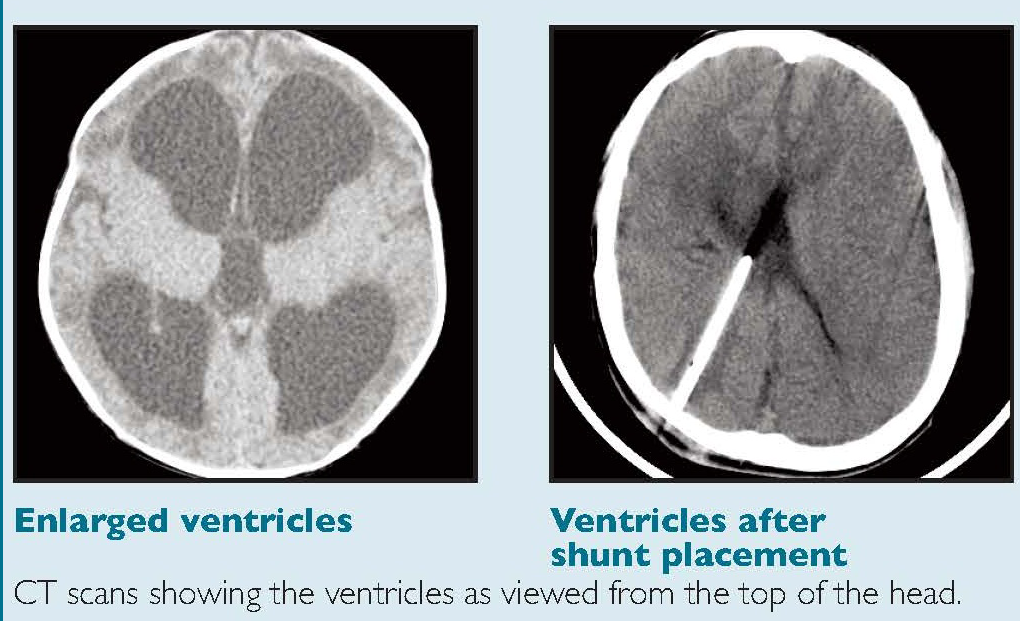
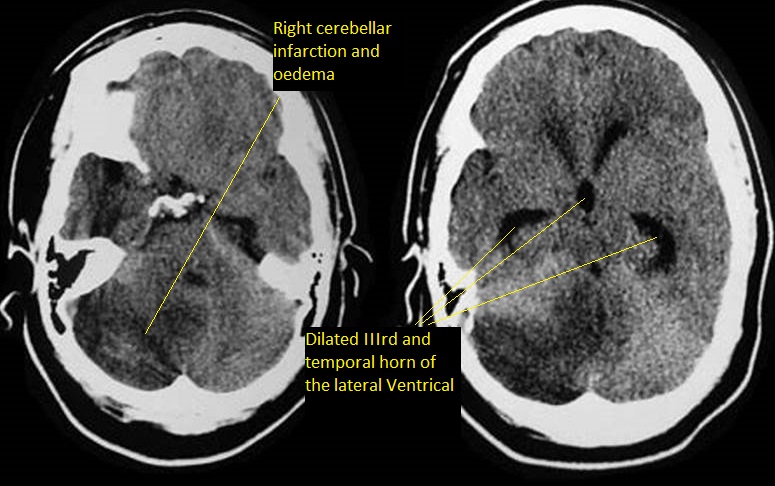
- CT head = key ➝ dilated ventricles (earliest: temporal horns rounded/expanded).
- MRI: more detailed; defines level & cause of obstruction.
- Look for mass effect, posterior fossa oedema, intraventricular blood, midline shift, periventricular oedema.
💊 Management
- Some mild hydrocephalus resolves spontaneously ➝ observe closely.
- Communicating hydrocephalus: LP may relieve pressure (if no obstructive lesion).
- ⚠️ Early neurosurgical referral essential if deteriorating.
- External ventricular drain (EVD): via burr hole ➝ drains CSF, lowers ICP.
- In SAH: reduce ICP gradually to avoid rebleeding.
- Shunting is difficult acutely due to high-protein/bloody CSF (shunt blockage risk).
📚 References & Further Reading
