Related Subjects:
|Causes of abnormal Vaginal bleeding
|Vaginal Carcinoma
|Cervical cancer
|Endometrial (Uterine) Cancer
|Post Menopausal Bleeding
|AP of the Uterus and Fallopian Tubes
|AP of the Ovary
|Gynaecological History Taking
|Colposcopy
|Premature Menopause
|Polycystic Ovary syndrome
Overview
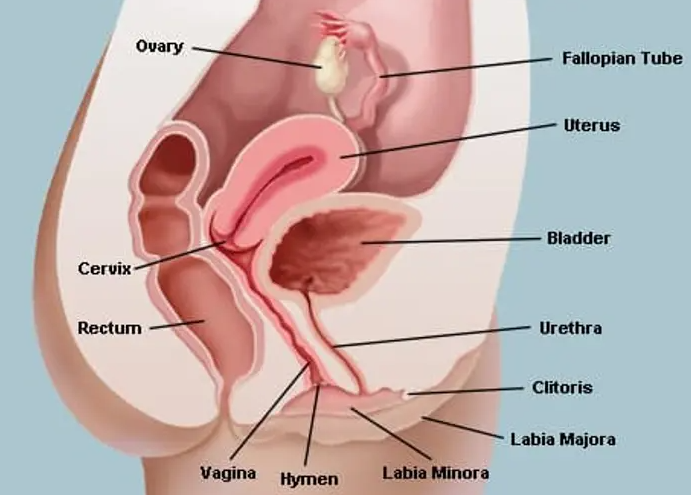
- The vagina is a fibromuscular canal extending from the vulva to the cervix, forming part of the lower female genital tract.
- Functions include sexual intercourse, menstrual outflow, and acting as the birth canal during vaginal delivery.
📍 Location and Relations
- Runs posterosuperiorly from the vestibule to the cervix (typically ~7–10 cm, variable).
- Anterior: bladder base and urethra.
- Posterior: rectum (upper posterior wall related to the pouch of Douglas/peritoneum).
- Lateral: levator ani and pelvic fascia; ureters lie close to the cervix (clinically relevant in surgery).
🧱 Gross Structure
- Upper end: surrounds the cervix to form the vaginal fornices (anterior, posterior, and two lateral).
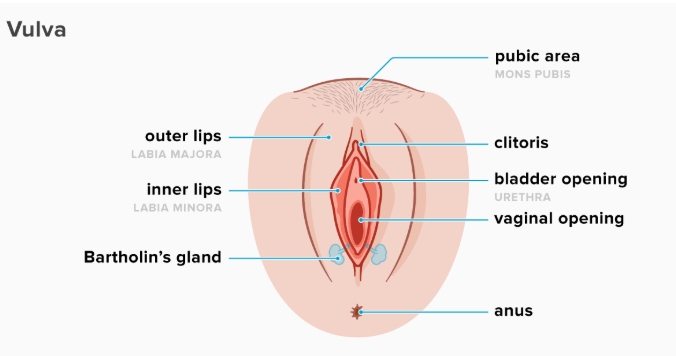
- Lower end: opens into the vaginal vestibule (between the labia minora).
- Anterior vs posterior walls: the posterior wall is usually longer due to the cervix position.
- The mucosa forms transverse folds called rugae (more prominent in premenopausal states).
🔬 Histology
- Mucosa: stratified squamous non-keratinised epithelium (protective; no glands).
- Lamina propria: elastic fibres, venous plexuses, immune cells (local defence).
- Muscularis: smooth muscle (inner circular + outer longitudinal) with variable thickness.
- Adventitia: connective tissue anchoring to pelvic structures; contains vessels and nerves.
- No vaginal glands: lubrication mainly from cervical mucus and transudation through the vaginal wall; vestibular glands contribute to vulval lubrication.
🩸 Blood Supply
- Arterial supply: predominantly from the vaginal artery (branch of internal iliac) and contributions from the uterine artery and internal pudendal artery.
- Venous drainage: vaginal venous plexus → internal iliac veins (rich venous plexus can bleed significantly with trauma).
🧠 Nerve Supply
- Upper vagina (autonomic): visceral afferents via the uterovaginal plexus (inferior hypogastric plexus) → pain tends to be poorly localised.
- Lower vagina (somatic): via pudendal nerve → touch/pain is well localised (important for procedures and childbirth pain).
🧬 Lymphatic Drainage
- Upper vagina: internal iliac ± external iliac nodes.
- Middle vagina: internal iliac nodes.
- Lower vagina and introitus: superficial inguinal nodes.
- Clinically important for vaginal and cervical malignancy staging and patterns of spread.
🏗️ Support and Pelvic Floor Relations
- Supported by the levator ani (especially pubococcygeus/puborectalis), perineal body, and endopelvic fascia.
- The perineal body is a key fibromuscular node (injury can contribute to pelvic organ prolapse).
⚙️ Physiology
- Vaginal environment: usually acidic in reproductive years (typically pH ~3.8–4.5).
- Oestrogen effect: increases epithelial thickness and glycogen content.
- Lactobacilli metabolise glycogen → lactic acid → maintains acidity and inhibits pathogens.
- Lubrication: largely via plasma transudate during arousal plus cervical secretions; integrity depends on oestrogen and mucosal health.
- Mechanical roles: distensible canal allowing intercourse and childbirth; rugae and elastic tissue support expansion and recoil.
🔄 Changes Across the Lifespan
- Prepubertal: thin epithelium, neutral/alkaline pH, reduced lactobacilli → higher infection/irritation susceptibility.
- Reproductive years: oestrogenised thick mucosa, acidic pH, prominent rugae, robust microbiome.
- Postmenopausal: low oestrogen → thin fragile mucosa, reduced glycogen/lactobacilli, higher pH → dryness, dyspareunia, and vulnerability to inflammation/UTI symptoms (often termed GSM).
🩺 Clinical Correlates
- Speculum examination: uses the distensibility and fornices; posterior fornix relates to the pouch of Douglas (site for fluid collection).
- Infection defence: acidity and lactobacilli are central-antibiotics, semen (alkaline), bleeding, and low oestrogen can alter pH and microbiome.
- Trauma/bleeding: rich venous plexus + mucosal fragility in low oestrogen states can make bleeding more likely.
- Lymph drainage patterns help explain node involvement in malignancy and guide assessment.
🧠 Teaching Commentary (Makindo-style)
- Think of the vagina as a hormone-responsive, immunologically active mucosa: oestrogen thickens epithelium and loads it with glycogen, which “feeds” lactobacilli to maintain an acidic pH-this is a key reason infection patterns differ prepubertally and postmenopausally.
- The upper vs lower innervation split matters clinically: upper vagina pain is visceral (vague), while the lower third is pudendal (sharp/well localised), explaining why procedures at the introitus often need more targeted local anaesthesia.
- Remember there are no vaginal glands; most lubrication is transudate plus cervical/vestibular contributions-so low oestrogen states disproportionately cause dryness and microtrauma.
