Related Subjects:
|Dilated Cardiomyopathy
|Hypertrophic cardiomyopathy (HCM - HOCM)
|Peripartum cardiomyopathy
|Restrictive Cardiomyopathy
|Takotsubo Cardiomyopathy
🫀 Broken Heart Syndrome (Takotsubo Cardiomyopathy) is a stress-induced, reversible cardiomyopathy.
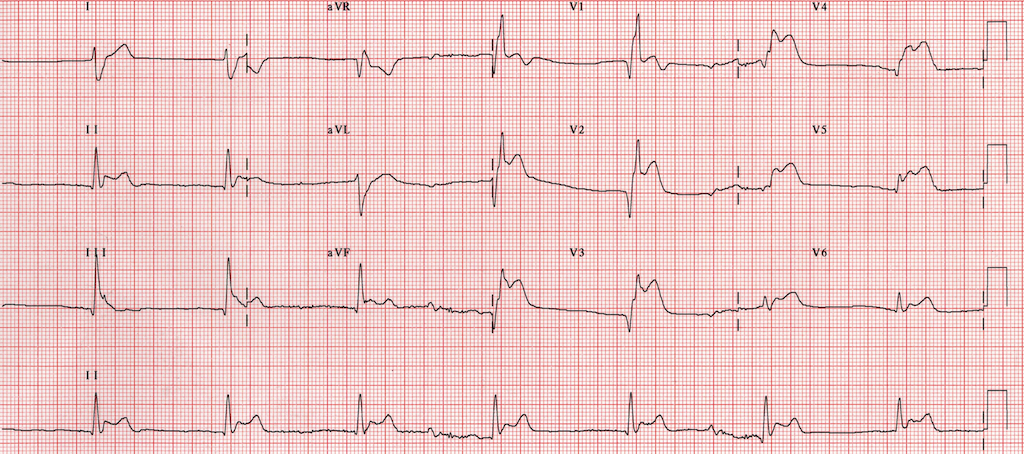
It mimics ACS with chest pain, dyspnoea, and ECG changes, but lacks significant coronary obstruction.
Most patients recover fully within days–weeks, but early recognition is crucial to avoid complications.
📖 About
- A retrospective diagnosis → always manage initially as ACS.
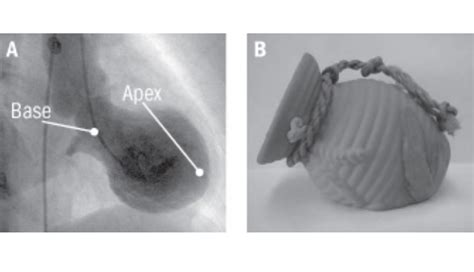
- Characterised by apical ballooning of the LV, giving the “takotsubo” shape (Japanese octopus trap).
- Described in 1990 (Japan). Mimics STEMI but angiography shows no obstructive CAD.
- Triggered by severe emotional or physical stress → hence “broken heart syndrome.”
- 90% are post-menopausal women, particularly of Asian or Caucasian origin.
🧬 Aetiology
- Likely due to catecholamine surge (adrenaline/noradrenaline → direct myocardial stunning).
- Microvascular dysfunction and coronary spasm may contribute.
- Triggers: grief, trauma, surgery, infection, financial stress, or extreme exertion.
- Typically no coronary obstruction on angiography.
⚠️ Clinical Features
- Acute chest pain + dyspnoea (mimics MI).
- Can progress to cardiogenic shock, acute heart failure, or pulmonary oedema.
- Arrhythmias: AF, VT, or VF.
- LV thrombus formation or (rarely) free wall rupture.
- Often preceded by emotional or physical stressor.
🔎 Differential Diagnosis
- ACS (STEMI/NSTEMI)
- Myocarditis
- Acute heart failure
- Phaeochromocytoma (can mimic Takotsubo)
🧪 Investigations
- ECG: ST elevation, T-wave inversion, QT prolongation, or non-specific changes (STEMI mimic).
- Echocardiography: Apical akinesis + basal hyperkinesis → “apical ballooning.”
- Troponin: Mild/moderate rise (lower than STEMI).
- BNP: Often markedly raised.
- Coronary angiography: Normal or non-obstructive coronary arteries.
- Cardiac MRI: Confirms diagnosis; no late gadolinium enhancement (no infarct scar).
- Catecholamines: Often very high compared to STEMI.
💊 Management
- Initial: Treat as ACS (Aspirin, β-blocker, ACEi) until Takotsubo is confirmed.
- Supportive: O₂, diuretics if pulmonary oedema, manage arrhythmias.
- Anticoagulation if LV thrombus or severe LV dysfunction.
- β-blockers → reduce catecholamine effect, esp. if LVOT obstruction.
- ACEi/ARB → aid LV recovery.
- LV function usually recovers in 1–4 weeks → repeat echo to confirm.
📉 Prognosis
- Generally excellent → complete recovery in most cases.
- 10% recurrence risk; long-term follow-up advised.
- Complications: cardiogenic shock, arrhythmias, LV rupture.
- Psychological support often beneficial (stress trigger link).
📚 References
