Related Subjects:
|Herpes Varicella-Zoster (Shingles) Infection
|Herpes Viruses
|Herpes Zoster Ophthalmicus (HZO) Shingles
|MonkeyPox
|Mumps
|Measles
|Rubella (German Measles)
|Epstein-Barr Virus infection
|Cytomegalovirus (CMV) infections
|CMV retinitis infections
|Toxoplasmosis
|Respiratory Failure
🧠 Guillain-Barré Syndrome (GBS): Respiratory function must always be monitored, as failure may occur silently without dyspnoea.
⚠️ Around 20% of patients need mechanical ventilation.
📏 Bedside test = Forced Vital Capacity (FVC); <1.5 L suggests ITU admission.
💉 IVIG within 2 weeks of onset is as effective as plasma exchange (Cochrane review) and more likely to be completed.
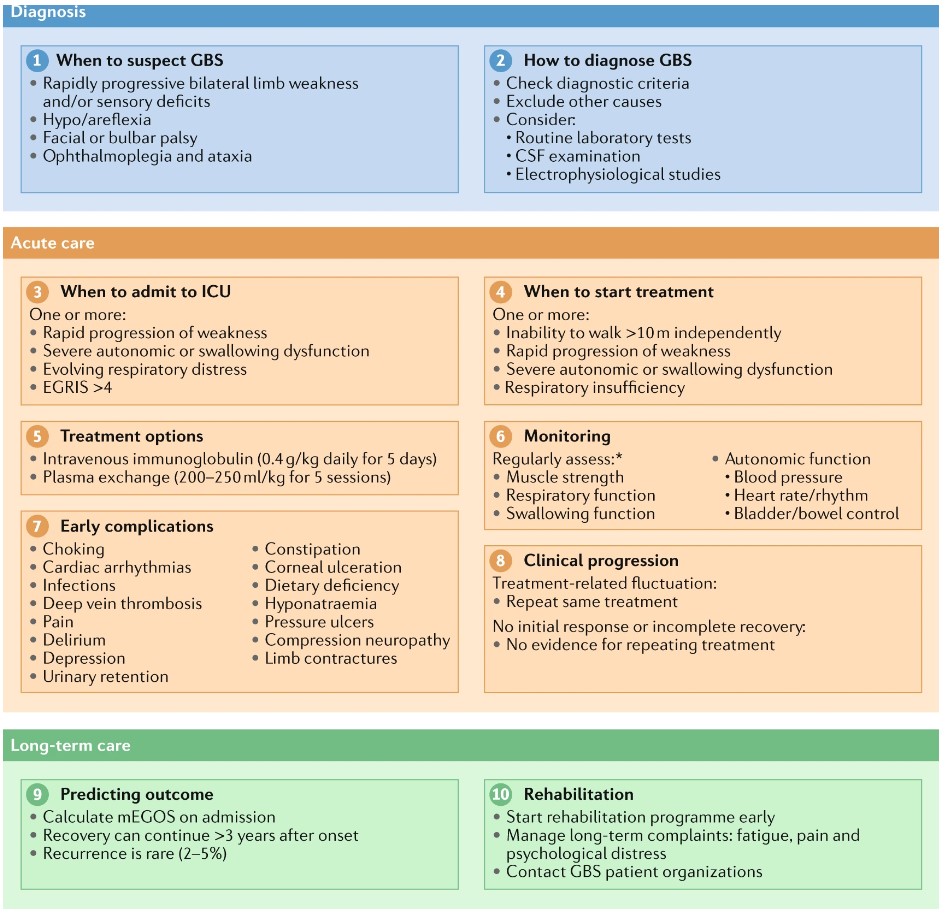
🩺 Initial Management of GBS
| Initial Priorities |
|---|
- 🔄 ABC assessment. ITU if FVC <15–20 ml/kg or <1 L, abnormal ABG, or hypoxia.
- ⚡ Confirm with nerve conduction studies (e.g., absent F waves).
- 💉 IVIG 0.4 g/kg for 5 days if significant weakness present.
- 🛡️ VTE prophylaxis, skin care, bowel & bladder management.
- 🥤 IV fluids, NG/PEG if swallowing unsafe.
- 🫁 Regular FVC monitoring to anticipate respiratory decline.
|
📖 About
- Acute onset ascending weakness + areflexia 🔽.
- Potentially life-threatening due to autonomic or respiratory failure.
- Also called Acute Inflammatory Demyelinating Polyneuropathy (AIDP).
🧬 Aetiology
- ⚔️ Autoimmune attack against peripheral nerves (molecular mimicry).
- 🌱 Infectious triggers: Campylobacter jejuni, CMV, HIV, HEV, EBV, Mycoplasma, Zika, Lyme.
- Pathology: multifocal demyelination + high CSF protein (albuminocytologic dissociation).
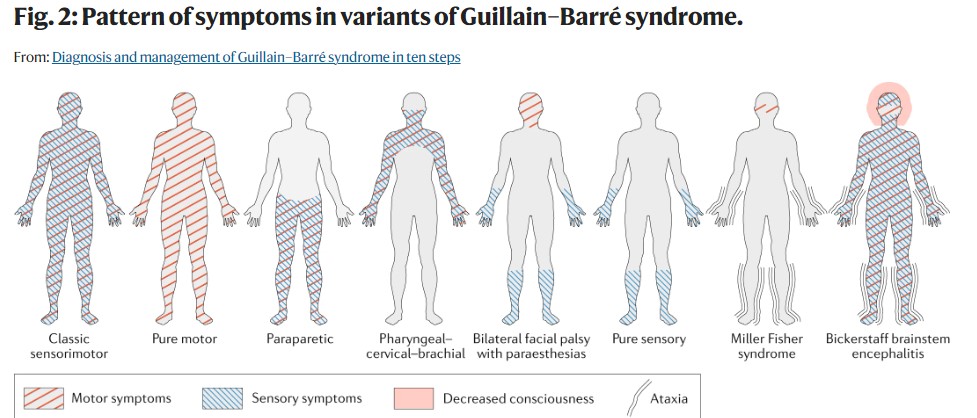
🔎 Subtypes of GBS
- AIDP (90%) – classic form, demyelinating.
- AMAN (5%) – acute motor axonal neuropathy, often after Campylobacter.
- Miller-Fisher (5%) – triad: ophthalmoplegia 👁️, ataxia 🚶, areflexia.
- AMSAN (1%) – motor + sensory axonal neuropathy.
⚠️ Clinical Features
- 🔼 Ascending weakness (legs → trunk → arms → cranial nerves).
- ❌ Areflexia.
- 🫁 Respiratory weakness ± need for ventilation.
- ❤️ Dysautonomia: BP swings, arrhythmias, pupillary changes.
- 🩻 Back pain, sensory loss, cranial neuropathies.
- 👀 Papilloedema possible due to high CSF protein.
🧪 Investigations
- 🧫 CSF: Protein ↑, normal WCC (may be normal early).
- ⚡ NCS: Slowed conduction, absent F-waves, conduction block.
- 🫀 ECG: monitor for arrhythmias.
- 🧬 Antibody testing rarely useful (anti-GD1a, anti-GQ1b in Miller-Fisher).
🩻 Differentials
- Spinal cord lesions (transverse myelitis).
- Myasthenia gravis, botulism.
- Tick paralysis, diphtheria, poliomyelitis.
- Acute porphyria.
🚨 Indications for ITU/Intubation
- FVC <15–20 ml/kg or <1 L.
- 🫁 Abnormal inspiratory/expiratory pressures.
- ❌ Severe bulbar weakness or impaired cough.
- 📉 Autonomic instability or abnormal gases.
💊 Management
- Specific: IVIG (within 2 weeks) or plasma exchange (within 4 weeks). 🚫 Steroids ineffective.
- Supportive: ITU if required, VTE prophylaxis, physiotherapy, speech therapy, nutrition support.
- Pain: Neuropathic analgesia (gabapentin, carbamazepine). Avoid amitriptyline (arrhythmia risk).
📈 Outcome
- Most improve within 12 months, but recovery may continue up to 5 years.
- 85% recover well; 15% left with disability.
- Poor prognosis: rapid onset, older age, preceding diarrhoea, severe initial weakness.
⚠️ Complications
- Bulbar dysfunction → aspiration, malnutrition.
- Autonomic storms → arrhythmias, BP swings.
- Immobility → pressure sores, DVT/PE, infections.
📚 References
Cases - Guillain–Barré Syndrome (GBS)
- Case 1 - Classic Post-Infectious Ascending Weakness 🦵:
A 32-year-old man develops tingling in his feet one week after a Campylobacter gastroenteritis. Over 3 days, he develops progressive ascending weakness, now unable to climb stairs. Exam: bilateral foot drop, absent ankle reflexes, intact cranial nerves.
Diagnosis: Acute inflammatory demyelinating polyneuropathy (AIDP, most common GBS subtype).
Management: Admit for monitoring; IV immunoglobulin (IVIG) or plasma exchange; monitor vital capacity regularly.
- Case 2 - Miller–Fisher Variant 👁️:
A 45-year-old woman presents with acute diplopia and unsteady gait. Exam: ophthalmoplegia, ataxia, and areflexia, but normal limb strength. CSF shows albuminocytologic dissociation. Anti-GQ1b antibodies positive.
Diagnosis: Miller–Fisher variant of GBS.
Management: IVIG; supportive physiotherapy and rehabilitation.
- Case 3 - Severe GBS with Respiratory Involvement 🫁:
A 28-year-old man presents with progressive ascending weakness, facial diplegia, and dysphagia. Exam: bilateral flaccid paralysis, absent reflexes, reduced single-breath count.
Diagnosis: Severe GBS with bulbar and respiratory muscle involvement.
Management: Admit to ICU; intubation and ventilation if vital capacity falls; IVIG or plasma exchange; multidisciplinary supportive care.
Teaching Commentary 🧠
GBS is an acute, immune-mediated polyneuropathy triggered by infections (e.g. Campylobacter, EBV, CMV, HIV) or rarely vaccination.
Hallmarks: progressive symmetrical weakness (usually ascending), areflexia, mild sensory symptoms, autonomic instability (arrhythmias, BP swings).
Investigations:
- CSF: albuminocytologic dissociation (↑protein, normal cells).
- Nerve conduction: demyelination (slowed conduction, conduction block).
Complications: respiratory failure (20–30%), autonomic dysfunction.
Treatment: IVIG or plasma exchange (equally effective); steroids are not helpful. Monitor in hospital until clear plateau or recovery.
