Slipped Upper Femoral Epiphysis (SUFE)
Related Subjects:
|Developmental Dislocation (Dysplasia) of the Hip (DDH)
|Slipped Upper Femoral Epiphysis (SUFE)
|Perthes disease (Osteochondritis of the Hip)
|Avascular Necrosis of Femoral head
|Fractured Neck of Femur
|Fractured Shaft Femur
|Supracondylar Femur Fractures
|Femoral fractures and Injuries
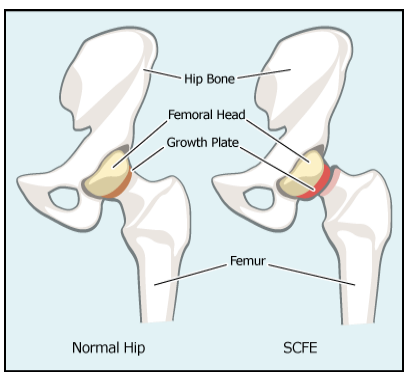
In SUFE the growth plates/epiphysis of the femoral head displaces or slips out of alignment from the rest of the femur. Hip pain in adolescent. It usually happens around puberty between the ages of 11 and 17 years and is more common in boys than girls. Refer immediately to orthopaedics. Needs X-rays AP and frog legs of BOTH hips.
ℹ️ About
- Affects mainly teenagers, obese children and boys
- May affect both hips so both need X Rayed
🧬 Aetiology
- SUFE is rare and is seen in 3/100,000.
- It is Bilateral in 25%
- Seen in teenagers during puberty
- Boys age 14-16, Girls 11-13
Risks
- Obesity, Male >Female 5:1
- Raised GH, Low sex hormones, hypothyroid
Clinical
- Adolescents: difficulty walking or a limp or limited movement
- There is Hip, groin or knee pain usually in adolescence
- A very reliable sign of a chronic SUFE, even when mild, is obligatory external rotation of the leg during hip flexion.
- Externally rotated, shortened, reduced abduction, increased adduction
- Patients are classified as having a stable or unstable slip based on their ability to weight bear on the affected
Differentials
- Septic arthritis
- Synovitis
- Osteomyelitis
🔎 Investigations
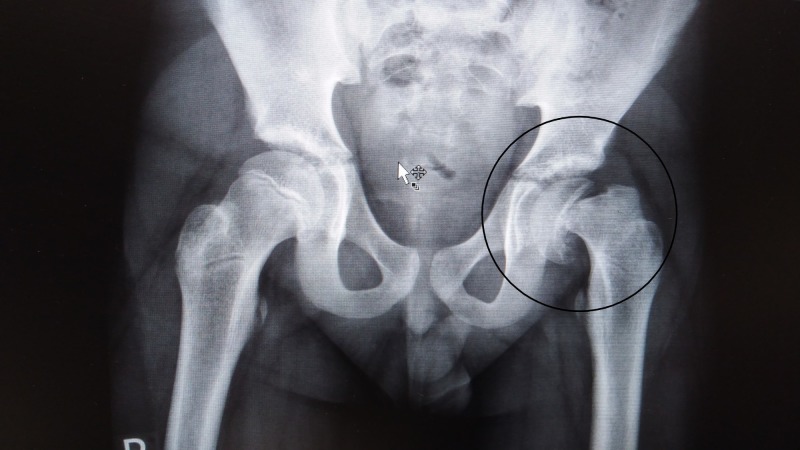
- X-ray: AP and lateral view of both hips. Radiographs (AP and frog leg) of the hip may show widening and irregularity of the physis with posterior inferior displacement of the femoral head.
- A Line drawn parallel to the femoral neck (Klein's line) will usually intersect with the lateral portion of the femoral epiphysis (Trethowan's sign).
- MRI scan may be needed
X-ray left hip with complete slippage of the epiphysis
💊 Management
- All patients with a SUFE or concern for a SUFE should be kept non-weight bearing and referred for an urgent orthopaedic assessment in the ED. The management of SUFE is always surgical. Analgesia and rest initially.
- SUFE may compromise the vascular supply to the femoral head and lead to avascular necrosis; all cases warrant urgent orthopaedic referral, and unstable SUFE should be referred emergently. Unstable SUFE has a much greater risk of avascular necrosis.
- Treatment includes non-weight bearing and surgery with epiphyseal fixation and possible osteotomy. Most patients do well after surgical fixation. Complications include avascular necrosis and chondrolysis.
- Patients require long term follow up as SCFE may develop within 12 to 18 months in the contralateral hip if prophylactic pinning is not performed
- Children who do not fit the typical profile for SCFE(under age 10 or over age 16, thin) should undergo evaluation for endocrinopathies (thyroid disease, growth hormone abnormalities) associated with SCFE
Surgery
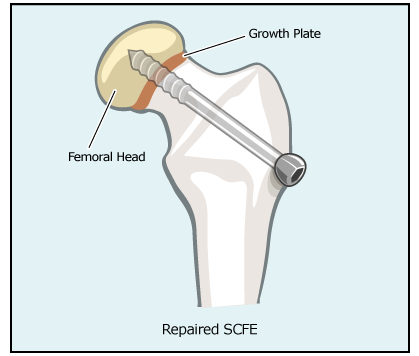
- A surgical screw is inserted across the growth plate securing it to the head of the. The child will be on bed rest for a few days and then non-weight bearing for 6 weeks. After about 2 weeks they will be seen in clinic to check their wounds are healing.
- They will see a physiotherapist, who will discuss any possible problems once at home and show them how to get around on crutches.
References
