Fractures in Children
🔗 Related Subjects:
| Osteomalacia – Rickets – Vitamin D
🦴 About
- Fractures occur in around 20% of children following injury.
- Lifetime risk of a fracture before age 16: Boys 42%, Girls 27%.
- Common sites: Distal radius, hand, elbow, clavicle, radius, tibia.
⚙️ Aetiology
- 💡 The epiphysis is the site of bone elongation and fuses in adulthood.
- 🧒 Children’s bones can absorb more energy before fracturing - they bow rather than break.
- 🩸 Excellent vascular supply → rapid healing and strong remodelling potential.
- ⚽ Mechanisms: sports injuries, falls, bike accidents, and road traffic collisions.
- 🥛 Risk increased by poor nutrition, calcium deficiency, or vitamin D deficiency.
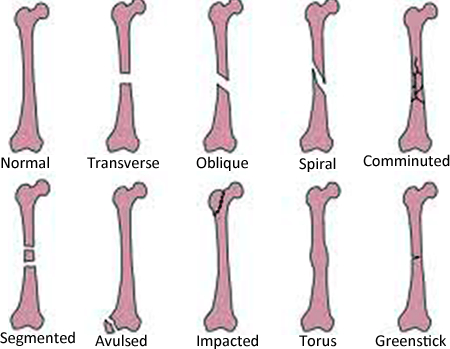
🔢 Types of Fractures in Children
- Single, non-displaced
- Transverse
- Oblique
- Spiral
- Comminuted (multiple fragments)
- Segmented
- Avulsion (chip of bone pulled off by tendon/ligament)
- Impacted
- 🔵 Torus fracture: buckling of cortex without complete break
- 🟢 Greenstick fracture: one cortex broken, the other intact
- 🔴 Open fracture: bone communicates with the exterior through the skin
🦵 Common Fracture Sites
- Clavicle: Middle third (80%); due to FOOSH, shoulder fall, or direct blow.
- Humerus: Midshaft rare; distal humeral (supracondylar) fractures common.
- Elbow: ~10% of all paediatric fractures; often supracondylar - immobilise before X-ray to prevent neurovascular injury. Flexion 20–30° minimises nerve tension.
- Radius/Ulna: Common after FOOSH; both bones often fractured together.
- Distal Radius: Most common childhood fracture; peaks at growth spurts (Boys 13–14, Girls 11–12).
- Wrist: Carpal fractures rare under age 12; scaphoid fractures seen in adolescents.
- Hand: Phalangeal/metacarpal injuries due to crush, twist, or sports trauma.
- Tibia/Fibula: Often occur together; twisting or fall mechanism.
- Toddler’s fracture: Spiral tibial fracture in <3-year-olds learning to walk; often subtle, child refuses to weight-bear.
- Ankle: Sports or play injuries - inversion/eversion strains common.
- Foot: Minor in most cases; calcaneal or tarsal fractures after falls.
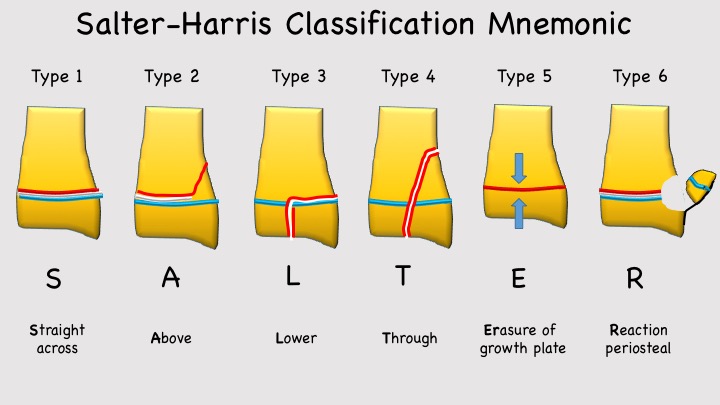
📊 Fractures Through the Epiphysis – Salter-Harris Classification
- ⚽ Mechanism: Usually sports injuries but may occur in abuse, metabolic or neurological disorders.
- Type I: Through the physis only - epiphysis separates from metaphysis.
- Type II: Through the metaphysis and physis (most common).
- Type III: Through physis and epiphysis - intra-articular (e.g. Tillaux fracture).
- Type IV: Through metaphysis, physis, and epiphysis - risk of growth arrest.
- Type V: Crush injury of growth plate → poor prognosis, may cause bone growth arrest.
- 📉 Rare higher types (VI–IX) involve periosteum or metaphyseal bone loss.
🩺 Clinical Assessment
- Take careful history: mechanism, timing, and consistency with developmental stage.
- ⚠️ Always consider non-accidental injury - pattern, delay in presentation, inconsistent story.
- Inspect for swelling, redness, deformity, or open wounds.
- Compare to opposite limb.
- Assess joints above and below.
- Check neurovascular status (sensation, pulses, capillary refill).
- Test active and passive movement - pain and restriction guide location.
🔬 Investigations
- 🧫 Bloods: Calcium, phosphate, vitamin D (if osteomalacia/rickets suspected).
- 🩻 Radiology:
- Request precise region - forearm ≠ wrist ≠ hand.
- Always correlate clinically; imaging is not a substitute for examination.
- Follow-up X-rays as bone may remodel or displacement may become visible later.
⚕️ Management Principles
- 🦵 Children heal rapidly due to active periosteum; most fractures treated with casting or splinting.
- 🔩 Severe or displaced fractures may require internal fixation (plates/screws).
- 🧬 Growth plate injuries risk deformity or limb-length discrepancy → careful long-term follow-up.
- Re-examine in 7–10 days; repeat radiographs at 6–12 months if growth arrest suspected.
- 🚨 Entrapped periosteum may prevent reduction - MRI may be needed.
🔩 Management by Salter-Harris Type
- Type I–II: Closed reduction + cast/splint.
- Type III–IV: Open reduction and internal fixation (avoid crossing physis).
- Type V: Often missed initially; poor prognosis; refer urgently to orthopaedics.
📚 References
💡 Teaching tip: Children’s bones are resilient but still vulnerable - they bend before they break, and remodel rapidly once aligned.
Always think “growth plate, mechanism, and safeguarding.” 🧠
