| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Disseminated Intravascular Coagulation (DIC)
Related Subjects: |Microangiopathic Haemolytic anaemia |Haemolytic anaemia |Immune (Idiopathic) Thrombocytopenic Purpura (ITP) |Thrombotic Thrombocytopenic purpura (TTP) |Haemolytic Uraemic syndrome (HUS) |Thrombocytopenia |Disseminated Intravascular Coagulation (DIC)
⚠️ Disseminated intravascular coagulation (DIC) is a life-threatening clinicopathological syndrome. It arises from widespread activation of coagulation, generating fibrin clots that cause organ dysfunction, while consuming platelets and clotting factors → paradoxical bleeding + thrombosis. 💀 Classic teaching: “DIC = Death Is Coming”.
📖 About
- Seen in ~1% of hospital inpatients, usually in the context of severe underlying illness (e.g., ICU patients).
- Characterised by uncontrolled coagulation → consumption of clotting factors → bleeding diathesis.
- Results in massive haemorrhage, microthrombi, multi-organ failure; prognosis is poor and depends on reversing the trigger.
🦠 Important Causes
- Sepsis – most common; esp. Gram-negative, but also Gram-positive, viral (e.g., COVID-19, HIV, CMV), fungal, parasitic (malaria).
- Trauma & tissue injury – major trauma, burns, crush injuries, snake bites.
- Malignancy – acute promyelocytic leukaemia (APL/M3), solid tumours with metastases.
- Obstetric catastrophes – amniotic fluid embolism, placental abruption, severe pre-eclampsia/eclampsia, HELLP syndrome.
- Other: severe liver failure, massive transfusion/ABO incompatibility, vasculitis, aneurysms, heatstroke, recreational drugs.
🧬 Pathophysiology
- Excess thrombin generation → widespread fibrin clots in microvasculature.
- Consumption of fibrinogen, clotting factors (esp. II, V, VIII), and platelets.
- Platelet trapping → thrombocytopenia.
- Secondary hyperfibrinolysis → elevated fibrin degradation products (FDPs)/D-dimer.
🩺 Clinical Features
- Typically in critically ill patients (e.g., ICU, sepsis, trauma).
- Bleeding: oozing from IV sites/wounds, mucosal (mouth/GI), haematuria, epistaxis, intracerebral haemorrhage.
- Microvascular thrombosis → digital ischaemia, purpura fulminans, organ failure (renal, hepatic, pulmonary, CNS).
- Respiratory failure: ARDS on CXR in severe cases.
🔬 Investigations
- Platelets: usually <50–100 ×10⁹/L (often <50 in overt DIC).
- PT, APTT: prolonged.
- Fibrinogen: low (<1 g/L in overt cases; Clauss method preferred).
- Factor VIII/vWF: often reduced (consumed).
- ↑ FDPs / D-dimer (key fibrinolysis markers; very high in acute DIC).
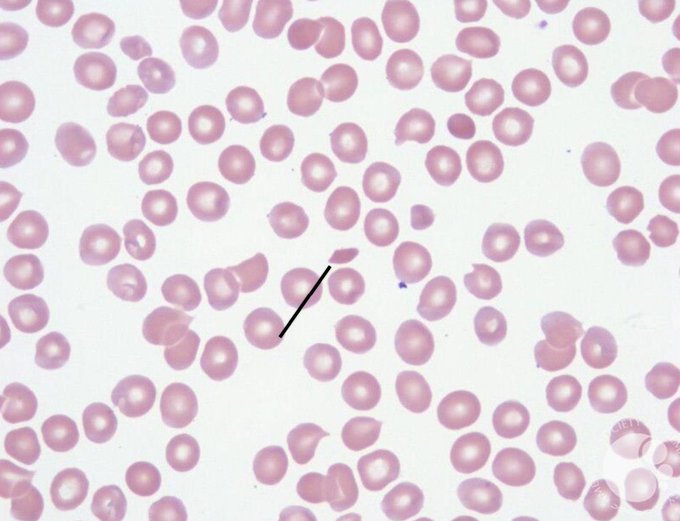
- Blood film: schistocytes (fragmented RBCs from microangiopathic haemolysis).
- CXR: may show ARDS pattern.
📊 Scoring System (Overt DIC – ISTH)
- Platelet count: >100 = 0; 50–100 = 1; <50 = 2.
- Fibrin markers (D-dimer/FDPs): no increase = 0; moderate increase (>3× upper limit) = 2; strong increase (>7× upper limit or ≥5× in classic) = 3 (ISTH 2025 refinement uses D-dimer thresholds).
- PT prolongation: <3s = 0; 3–6s = 1; >6s = 2 (or INR equivalent).
- Fibrinogen: >1 g/L = 0; <1 g/L = 1.
- Score ≥5 = compatible with overt DIC (repeat daily). <5 = suggestive of non-overt DIC (repeat every 1–2 days, monitor clinically).
📌 Differentials
- Thrombotic thrombocytopenic purpura (TTP).
- Haemolytic uraemic syndrome (HUS).
- HELLP syndrome / severe pre-eclampsia.
- Severe malignant hypertension.
- Liver failure / vitamin K deficiency (isolated coagulopathy).
🩸 Blood Film: Schistocytes
💊 Management (always involve Haematology urgently)
- 1. Treat the underlying cause aggressively – this is the cornerstone (e.g., antibiotics for sepsis, delivery/evacuation in obstetrics, ATRA/chemotherapy in APL, source control in trauma).
- 2. Supportive measures (transfusion only if bleeding or high-risk):
- Active bleeding or invasive procedure → platelets if <50 ×10⁹/L (target >50); FFP 15 mL/kg if PT/APTT prolonged.
- Low fibrinogen (<1 g/L) with bleeding → cryoprecipitate (or fibrinogen concentrate) to target >1–1.5 g/L.
- Monitor response: repeat platelets, PT/APTT, fibrinogen post-replacement.
- 3. Thrombosis-predominant DIC: consider therapeutic heparin (e.g., purpura fulminans, acral ischaemia) if no contraindications.
- 4. Non-bleeding critically ill patients: standard VTE prophylaxis with LMWH if appropriate.
- Avoid routine prophylactic transfusions based on labs alone (per BSH/ISTH). Consider Pabrinex (thiamine) in at-risk patients (e.g., alcoholics/sepsis) to prevent Wernicke's encephalopathy.
🔑 Think of DIC in any septic, bleeding, or rapidly deteriorating ICU patient. 💡 Labs: low platelets + prolonged PT/APTT + high D-dimer + low fibrinogen = classic pattern. 📉 Prognosis depends on reversing the underlying trigger – supportive therapy alone is insufficient.
📚 Reference
- British Society for Haematology (BSH): Guidelines for diagnosis & management of DIC (2009, addendum 2012 – current UK standard)
- ISTH SSC on DIC: Overt scoring system (2001, with 2025 refinements to D-dimer thresholds)
- No specific NICE guideline for DIC; refer to related pathways (e.g., NG51 sepsis, CG144 VTE).
Cases - Disseminated Intravascular Coagulation (DIC)
- Case 1 - Obstetric Emergency: A 32-year-old woman presents with massive postpartum haemorrhage following placental abruption. She is hypotensive and oozing blood from venepuncture sites. Bloods show platelets 45 ×10⁹/L, PT and APTT prolonged, fibrinogen very low, D-dimer markedly elevated. Diagnosis: Acute DIC secondary to obstetric catastrophe.
- Case 2 - Sepsis-Associated DIC: A 70-year-old man with pneumonia becomes hypotensive and develops mottled skin and purpura fulminans. He has active bleeding from his nasogastric tube. FBC: platelets 30 ×10⁹/L, Hb 7.8 g/dL. Coagulation profile: prolonged PT/APTT, low fibrinogen, high fibrin degradation products. Diagnosis: Sepsis-induced DIC.
- Case 3 - Malignancy-Related Chronic DIC: A 65-year-old woman with known metastatic pancreatic cancer presents with bruising, mucosal bleeding, and recurrent venous thromboembolism despite anticoagulation. Platelets are 80 ×10⁹/L, fibrinogen borderline low, PT mildly prolonged, D-dimer persistently elevated. Diagnosis: Chronic DIC in the context of malignancy.
Teaching Commentary 🩸
DIC is a pathological activation of the coagulation cascade, leading to simultaneous thrombosis and bleeding. In acute settings (e.g., sepsis, trauma, obstetrics), rapid consumption causes life-threatening bleeding. In chronic forms (e.g., malignancy), thrombosis may predominate with subtler bleeding. Diagnosis combines clinical context + labs: thrombocytopenia, prolonged PT/APTT, hypofibrinogenaemia, raised D-dimer. Management prioritises treating the underlying cause, with targeted supportive transfusion for bleeding and cautious anticoagulation if thrombosis dominates (BSH/ISTH guidance).