
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Hepatitis C
Related Subjects: | Chronic liver disease | Cirrhosis | Alkaline phosphatase (ALP) | Liver Function Tests | Ascites Assessment and Management | Budd-Chiari syndrome | Autoimmune Hepatitis | Primary Biliary Cirrhosis | Primary Sclerosing Cholangitis | Wilson disease | Hereditary Haemochromatosis | Alpha-1 Antitrypsin (AAT) deficiency | Nonalcoholic steatohepatitis (NASH) | Spontaneous Bacterial Peritonitis | Alcoholism and Alcoholic Liver Disease |Hepatitis C
💉 PEG = polyethylene glycol, a water-soluble polymer added to interferon to make it longer-acting. The goal is to eradicate HCV, prevent fibrosis, and reduce the risk of hepatocellular carcinoma (HCC). ⚠️ HCV is curable today with modern direct-acting antivirals (DAAs).
📖 About Hepatitis C
- 🦠 A viral infection causing chronic hepatitis and progressive liver damage.
- 🌍 Affects ~185 million people worldwide.
- 🚨 Leads to cirrhosis, liver failure, and HCC if untreated.
- 🇬🇧 UK: 200,000–400,000 infected, many undiagnosed and asymptomatic.
- Genotypes 1a & 1b common in Europe/US → harder to treat.
🧬 Aetiology & Pathophysiology
- RNA flavivirus with 6 genotypes. Genotype 1 = most common in Europe.
- 80% progress to chronic hepatitis → persistently abnormal LFTs.
- ~30% develop cirrhosis; ~5% develop HCC.
- Immune response determines outcome:
- Th1 response (γ-IFN, IL-2) → viral clearance.
- Th2 response (IL-4, IL-10, IL-13) → chronicity.
🔄 Transmission
- 💉 Blood transfusions/products (before screening protocols).
- 💊 IV drug use (most common in UK).
- 🤰 Maternal (vertical) transmission.
- ❤️ Sexual transmission (rare).
- 🩺 Needlestick injuries in healthcare workers.
👩⚕️ Clinical Features
- Acute infection → usually silent/asymptomatic.
- Chronic infection → fatigue, malaise, jaundice, dark urine, anorexia, nausea.
- Skin/extrahepatic features: purpura, vasculitis, neuropathy, cryoglobulinaemia.
- Associated with porphyria cutanea tarda & glomerulonephritis.
- ⚠️ Advanced disease → cirrhosis, portal hypertension, HCC.
🧪 Investigations
- ✅ Anti-HCV antibody (first-line screening).
- ✅ HCV RNA PCR (confirms infection, monitors treatment response).
- 🧬 Genotype testing → guides therapy choice.
- 📈 LFTs: mild ↑ ALT/AST (50–200).
- 🔬 Liver biopsy or elastography → assess fibrosis/cirrhosis.
- 🧫 Rheumatoid factor, cryoglobulins, low complement → extrahepatic features.
- 🧲 Imaging (US, CT, MRI) → cirrhosis/HCC surveillance.
⚠️ Risk Factors for Cirrhosis
- 🍺 Alcohol consumption.
- 🧑🦱 Male sex, age >40 at infection.
- 🦠 Co-infection with HIV or HBV.
- 💊 Immunosuppression.
🩺 Associated Conditions
- Porphyria cutanea tarda.
- Glomerulonephritis, diabetes, arthritis.
- Sicca syndrome, non-Hodgkin lymphoma.
- Lichen planus, cryoglobulinaemia.
💊 Management
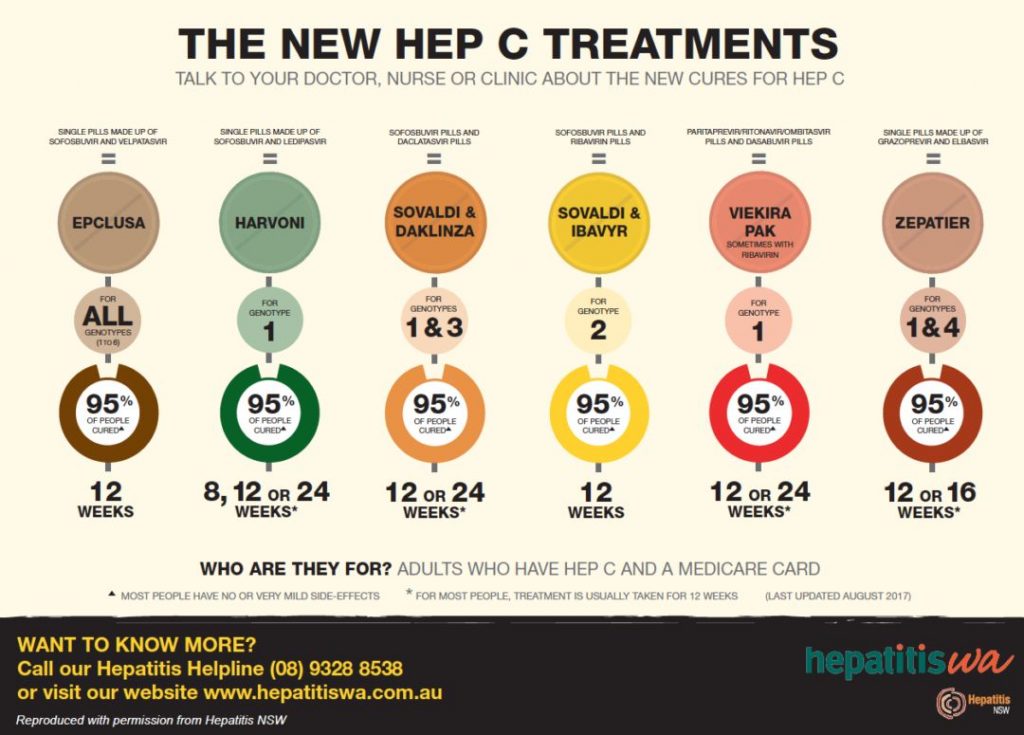
- 🎯 Direct-acting antivirals (DAAs) → >90% cure rates.
- Sofosbuvir (polymerase inhibitor, pan-genotype).
- Velpatasvir (NS5A inhibitor, used with sofosbuvir).
- Simeprevir (protease inhibitor).
- Voxilaprevir (used in resistant cases).
- Duration: 8–24 weeks depending on genotype & fibrosis.
- 🧪 Monitor via PCR for sustained virological response (SVR = cure).
- 🩺 Liver transplant if decompensated cirrhosis, but reinfection risk exists.
📌 Key Teaching Pearls
- 🦠 HCV is now curable → early diagnosis is essential.
- 🚨 Always screen at-risk patients (IV drug use, transfusions pre-1991, HIV+).
- 🔄 No vaccine exists → prevention relies on harm reduction (needle exchange, safe blood supply).
- 🧑⚕️ Chronic HCV → major cause of liver transplantation in the UK/US.
📊 Response to therapy = normal ALT + undetectable HCV RNA (SVR). This is equivalent to a virological cure ✅
📚 References
🧫 Hepatitis C – Clinical Cases
- Case 1 – Chronic Infection Discovered Incidentally: A 44-year-old man attends for a routine insurance medical. LFTs show ALT 98 U/L and AST 85 U/L. He feels well and denies jaundice, but recalls past injecting drug use in his 20s. Ultrasound shows mild fatty change; hepatitis C antibody and RNA are both positive. FibroScan reveals F1–F2 fibrosis. Teaching point: Many HCV cases are asymptomatic until detected on screening. Assess fibrosis stage (elastography or biopsy), screen for coinfection (HIV, HBV), and start direct-acting antiviral (DAA) therapy, which now cures > 95%.
- Case 2 – Extrahepatic Manifestation: Cryoglobulinaemic Vasculitis: A 55-year-old woman with known chronic hepatitis C presents with fatigue, arthralgia, and a purpuric rash on the lower legs. Urinalysis shows microscopic haematuria and proteinuria. Bloods reveal low complement C4 and positive cryoglobulins. Teaching point: HCV can trigger immune complex small-vessel vasculitis due to circulating cryoglobulins. Management requires antiviral therapy plus immunosuppression if severe (e.g. rituximab). Always consider HCV in unexplained vasculitis or membranoproliferative GN.
- Case 3 – Post-Treatment Relapse and Cirrhosis: A 63-year-old man with compensated cirrhosis secondary to hepatitis C genotype 3 completed sofosbuvir-velpatasvir 12 months ago. He re-presents with malaise, ascites, and rising bilirubin. HCV RNA is again positive, indicating relapse. Teaching point: Relapse or reinfection may occur, particularly in patients with advanced fibrosis or ongoing risk factors. He requires reassessment for retreatment options, variceal screening, and hepatocellular carcinoma surveillance every 6 months by ultrasound ± AFP.
💡 Clinical pearl: Always check both HCV antibody and HCV RNA to confirm active infection. Modern DAAs (e.g. sofosbuvir, glecaprevir/pibrentasvir) achieve sustained virological response within 8–12 weeks - a remarkable shift from the interferon era. 🌟
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery