
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Meckel diverticulum ✅
Related Subjects: |Testicular Torsion |Paraphimosis |Meckel's diverticulum
📖 About
- Meckel’s Diverticulum = congenital true diverticulum of the ileum, due to incomplete obliteration of the vitelline (omphalomesenteric) duct.
- Located on the antimesenteric border of the ileum, usually within 2 feet of the ileocaecal valve.
- May contain ectopic gastric or pancreatic tissue → risk of ulceration, bleeding, or perforation.
📏 Rule of 2s
- Occurs in ~2% of the population.
- 2:1 male predominance.
- Within 2 feet of the ileocaecal valve.
- ~2 inches long.
- Only 2% symptomatic.
- Often presents before age 2.
🔬 Histology
- True diverticulum (all intestinal wall layers present).
- Frequently contains ectopic gastric mucosa → acid secretion → ulceration, bleeding.
- Occasional pancreatic tissue.
🩺 Clinical Presentation
- Children: Painless rectal bleeding (bright red or “currant jelly”), anaemia, sometimes intermittent abdominal pain.
- Adults: Small bowel obstruction, diverticulitis (mimics appendicitis), abdominal pain, or incidental finding.
- Rare: volvulus, intussusception, perforation → peritonitis (surgical emergency).
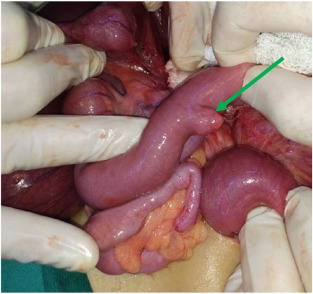
📷 Intraoperative Pictures

🧪 Investigations
- Technetium-99m Pertechnetate Scan (“Meckel’s scan”): highlights ectopic gastric mucosa; H2 blockers (e.g., ranitidine) increase sensitivity.
- CT/MRI/Ultrasound → detect complications (obstruction, intussusception, inflammation) but not specific.
- Full blood count, Hb, CRP, and coagulation if bleeding suspected.
⚕️ Management
- Symptomatic cases: Surgical resection (diverticulectomy ± segmental ileal resection); laparoscopic preferred when feasible.
- Incidental finding: Children → usually resect prophylactically. Adults → case-by-case based on risk factors (broad base, ectopic tissue, age, comorbidities).
- Perioperative: correct anaemia/volume status, prophylactic antibiotics per NICE/Trust protocol, early mobilisation post-op.
⚠️ Complications
- Bleeding – most common in children (from ectopic gastric mucosa).
- Obstruction – fibrous bands, intussusception, volvulus.
- Diverticulitis – mimics appendicitis.
- Perforation → peritonitis, urgent surgery.
- Recurrence or incomplete resection is rare but possible.
🌟 Prognosis
- Excellent outcome if resected when symptomatic.
- Most asymptomatic diverticula remain undetected lifelong.
- Prophylactic resection in adults remains controversial; guided by risk assessment and surgical judgement.
💡 Teaching Pearl: Meckel’s diverticulum is the most common congenital GI anomaly. Think of it in a child with painless rectal bleeding + normal colonoscopy → order a Meckel’s scan. NICE-compliant management emphasises prompt diagnosis, supportive care, imaging before surgery, and multidisciplinary discussion if adult resection is considered.
Case – Meckel’s diverticulum (bleeding child)
A 5-year-old boy presents with sudden, painless maroon rectal bleeding and mild pallor; no diarrhoea, fever, or abdominal pain. Vitals stable; abdomen soft, non-tender. Hb 9.6 g/dL, CRP normal. After IV access and fluid resuscitation, a Technetium-99m pertechnetate “Meckel scan” shows focal uptake in the right lower quadrant, consistent with ectopic gastric mucosa in a Meckel’s diverticulum. Differential considered: intussusception, juvenile polyp, infectious colitis. Managed with crossmatch ± transfusion if needed, then laparoscopic diverticulectomy (or segmental resection if broad base/ulceration). Post-op recovery uncomplicated; parents counselled on the “rule of twos” (2% prevalence, 2 feet from ileocaecal valve, 2 inches long, often symptomatic before age 2, 2 types of ectopic mucosa: gastric/pancreatic).
📚 References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery