
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Wolfram syndrome (DIDMOAD)
ℹ️ About
- 🧬 Wolfram syndrome (DIDMOAD) is a rare neurodegenerative disorder.
- 💡 Acronym: DIDMOAD = Diabetes Insipidus, Diabetes Mellitus, Optic Atrophy, and Deafness.
🧬 Aetiology
- 🧪 Caused by defects in the WFS1 gene (chromosome 4), leading to mitochondrial dysfunction and endoplasmic reticulum stress.
- 🔗 Less commonly linked to other nuclear or mitochondrial DNA mutations.
Features
- 💧 Diabetes Insipidus – impaired vasopressin secretion → polyuria & polydipsia.
- 🍬 Diabetes Mellitus – usually non-autoimmune, insulin-dependent onset in childhood.
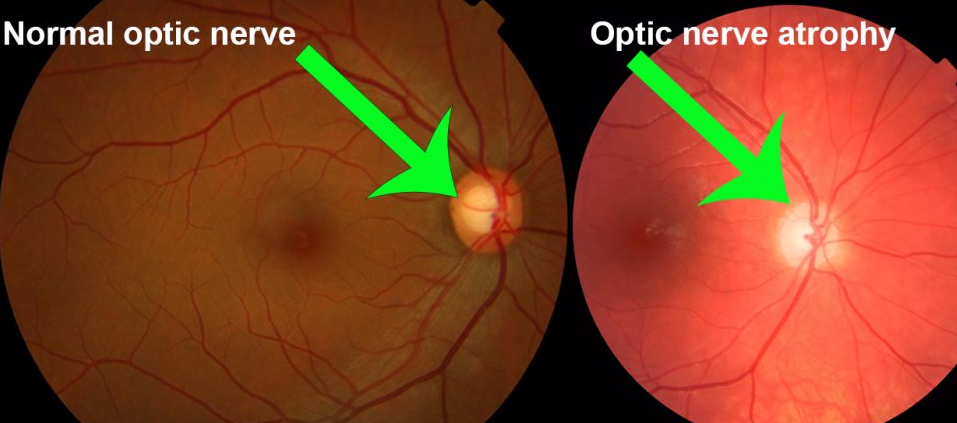
- 👁️ Optic atrophy – progressive loss of vision due to optic nerve degeneration.
- 🎧 Sensorineural deafness – often progressive, bilateral hearing loss.
🩺 Clinical Features
- 🧑🦱 Usually presents in childhood or adolescence.
- 💦 Polyuria and polydipsia from DI.
- 👓 Progressive visual loss (optic atrophy).
- 🔊 Hearing impairment due to SNHL.
- ⚠️ Other: ataxia, neuropathy, and psychiatric illness can develop in later stages.
🔎 Investigations
- 🩸 U&E: Hypernatraemia from uncontrolled DI.
- 🍭 Glucose: High plasma glucose confirms DM.
- 💉 Water deprivation test: Confirms central DI.
- 🧬 Genetic testing: WFS1 mutation analysis (definitive diagnosis).
💊 Management
- 💊 Symptomatic and supportive: manage DM with insulin, DI with desmopressin.
- 👁️ Ophthalmology: low-vision aids, regular monitoring of optic atrophy.
- 🎧 Audiology: hearing support (hearing aids/cochlear implant if needed).
- 🤝 Multidisciplinary care essential – endocrinology, neurology, ophthalmology, ENT, psychology.
📚 Exam tip: Remember DIDMOAD as the classic tetrad. The key distinction is that DM in Wolfram syndrome is non-autoimmune (unlike type 1 DM). Always think of Wolfram syndrome in a young patient with DM plus progressive vision and hearing loss. 🚨
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery