
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Accessory Nerve (Cranial Nerve XI)
Related Subjects: |Olfactory Nerve |Optic Nerve |Oculomotor Nerve |Trochlear Nerve |Trigeminal Nerve |Abducent Nerve |Facial Nerve |Glossopharyngeal Nerve |Vagus Nerve |Accessory Nerve
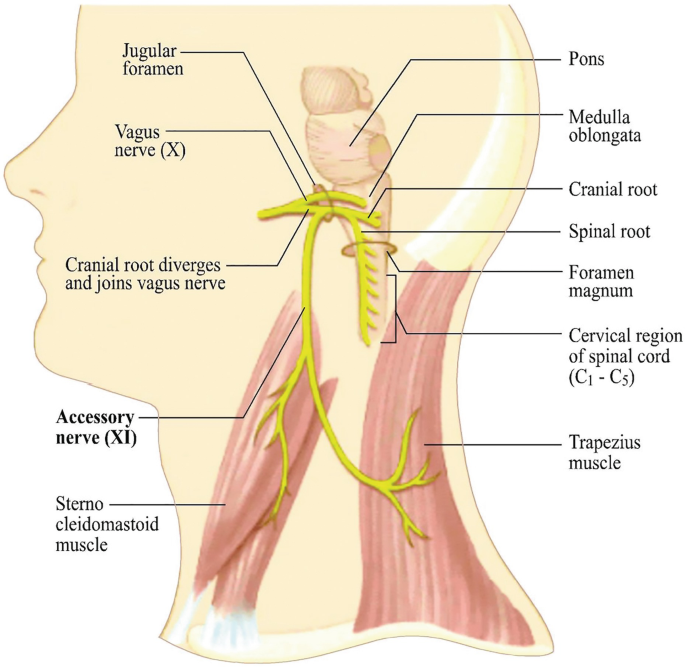
🧠 The accessory nerve (CN XI) is a predominantly motor cranial nerve supplying sternocleidomastoid (SCM) and trapezius. It is “special” because most of its fibres arise from the upper cervical spinal cord (the spinal accessory nucleus) and briefly enter the skull before exiting again. Clinically, it matters because CN XI is superficial in the posterior triangle of the neck-making it vulnerable during lymph node biopsy and neck surgery.
🧬 Core anatomy you must know
- Functional components
- Spinal part (the important bit clinically): motor to SCM + trapezius.
- Cranial part: often best thought of as joining the vagus (CN X) to contribute to palatal/pharyngeal/laryngeal motor function (many modern texts treat this “cranial root” as effectively vagal).
- Nuclei of origin
- Spinal accessory nucleus: ventral horn region of upper cervical cord (classically C1–C5/6).
- Cranial root: medulla (near nucleus ambiguus) → blends with vagus.
- Exit/entry points
- Spinal rootlets emerge laterally from cervical cord → ascend through the foramen magnum.
- Exits the skull via the jugular foramen (with CN IX and X, and the internal jugular vein).
🧭 Course (step-by-step, exam-friendly)
- 1) Cervical cord → skull
- Rootlets from C1–C5/6 converge → ascend into the posterior cranial fossa via foramen magnum.
- 2) Skull → neck
- Leaves through jugular foramen.
- Cranial fibres then merge with CN X; the “spinal accessory” continues as the nerve you test at the bedside.
- 3) Neck course & surgical danger zone
- Supplies SCM, then crosses the neck to the posterior triangle.
- Runs relatively superficial on/near levator scapulae deep to the investing fascia → vulnerable in:
- Posterior triangle lymph node biopsy
- Neck dissections (levels II–V)
- Penetrating trauma
- Then enters and supplies trapezius (often with contribution from cervical plexus proprioceptive fibres C3–C4).
💪 Actions: what CN XI actually does
- Sternocleidomastoid (SCM)
- Turns the head to the opposite side (right SCM turns face left).
- Assists with neck flexion.
- Important for “head-turn against resistance” testing.
- Trapezius
- Elevates scapula (shrug).
- Upwardly rotates scapula for arm elevation above shoulder height (works with serratus anterior).
- Stabilises scapula during pushing/pulling activities.
🩺 Examination (what to look for and why)
- Inspection first
- Shoulder asymmetry, droop, or wasting of trapezius.
- Scapular malposition; lateral scapular winging can occur in trapezius palsy (different from the classic medial winging of long thoracic nerve injury).
- Test trapezius
- Ask the patient to shrug shoulders against resistance.
- Assess strength and compare sides; palpate trapezius bulk.
- Ask patient to abduct the arm above 90°: trapezius weakness makes this hard due to reduced scapular upward rotation.
- Test SCM
- Ask the patient to turn head against your hand (e.g., turn left against resistance tests right SCM).
- Look for reduced turning power and SCM wasting.
🧠 Reasoning tip: Many CN XI lesions look “shoulder-dominant” because trapezius dysfunction is more disabling and more obvious than SCM weakness. If someone can still turn their head reasonably but has marked shoulder droop and difficulty abducting above 90°, think CN XI (trapezius) first.
🚑 Accessory nerve palsy: presentation and mechanisms
- Common causes
- Iatrogenic: posterior triangle lymph node biopsy, neck dissection, carotid surgery.
- Trauma: penetrating injury, traction.
- Compression/infiltration: tumours, lymphadenopathy, radiotherapy fibrosis.
- Key symptoms/signs
- Shoulder droop, pain, and fatigue (often prominent).
- Weak shoulder shrug.
- Difficulty abducting the arm above shoulder height.
- Scapular dyskinesis ± winging; trapezius wasting over time.
- Neck turning weakness if SCM involved.
🧪 Differentials (don’t miss)
- Long thoracic nerve palsy: serratus anterior weakness → medial scapular winging, worse with pushing against a wall.
- C5 radiculopathy: deltoid/biceps involvement, sensory changes, reflex changes.
- Brachial plexus / upper trunk lesion: broader motor deficits beyond trapezius/SCM.
- Rotator cuff pathology: pain-limited weakness, preserved shrug strength.
🧷 Investigations (when needed)
- Often clinical if classic post-surgical picture.
- EMG/NCS: confirms denervation and localises lesion; helpful if diagnosis unclear or prognostication needed.
- Imaging:
- Neck ultrasound/CT/MRI if tumour, mass, or unexplained progressive palsy.
- Shoulder imaging only if concomitant structural shoulder pathology suspected.
🛠️ Management (principles)
- Early physiotherapy
- Scapular stabilisation, range of motion, posture, pain control.
- Prevents secondary adhesive capsulitis and chronic pain syndromes.
- Treat the cause
- Address compressive lesions, tumour, or post-op complications.
- Surgical options (selected cases)
- Nerve repair/grafting if transection recognised early.
- Tendon transfers (e.g., Eden–Lange-type procedures) in chronic trapezius paralysis with functional limitation.
📌 Summary
CN XI is a motor nerve (predominantly spinal in origin) supplying SCM and trapezius. Its superficial course through the posterior triangle makes it vulnerable in neck surgery and lymph node biopsy. Clinically, palsy typically presents with shoulder droop, weak shrug, difficulty abducting above 90°, scapular dyskinesis/winging, and sometimes impaired head turning. A clear bedside exam, awareness of differentials (long thoracic nerve, C5 radiculopathy), and early physio are key to good outcomes.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery