Related Subjects:
| Resuscitation - Adult Tachycardia Algorithm
⚡ Automatic Implantable Cardioverter Defibrillators (ICDs) are recommended for people at high risk of sudden cardiac death (ventricular arrhythmias, inherited cardiac syndromes, congenital repair surgery).
They can deliver pacing, cardioversion, or defibrillation.
ICDs and CRT (cardiac resynchronisation therapy) improve survival in selected patients with LV dysfunction and heart failure.
📖 About
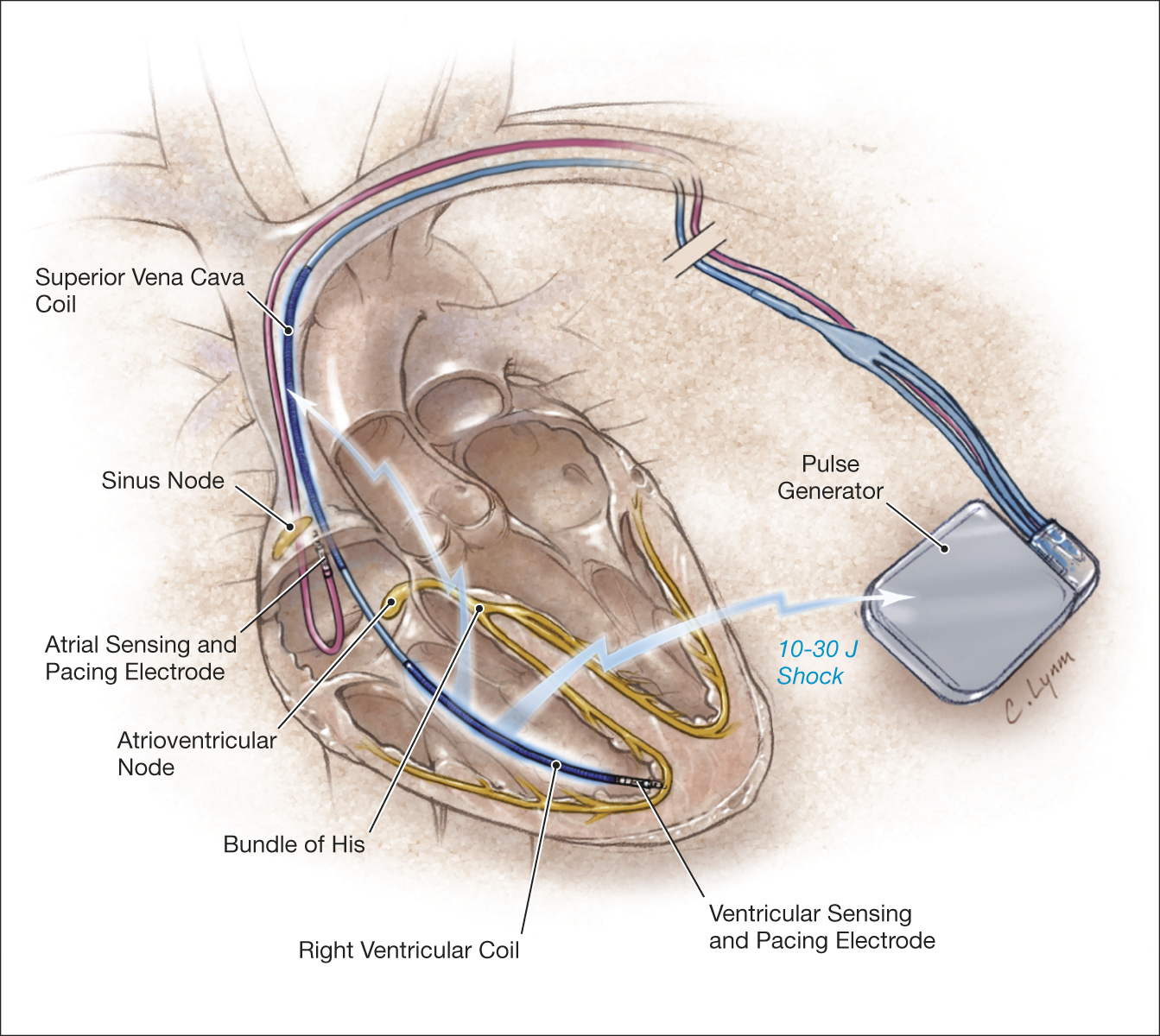
- ICD = device to treat ventricular tachycardia (VT) and ventricular fibrillation (VF).
- Implanted under the clavicle, slightly larger than a pacemaker.
- Contains a pulse generator + electrode leads (RA/RV ± SVC coil).
- Battery lasts 4–6 years (≈100 shocks).
⚙️ How It Works
- Monitors RR intervals for tachyarrhythmias.
- Responds with:
- ⚡ Pacing: rapid, low-voltage impulses (anti-tachycardia pacing).
- ⚡ Cardioversion: synchronised small shocks.
- ⚡ Defibrillation: large unsynchronised shock.
- Charging takes 6–15s → re-confirms rhythm before shock.
- ≈10% shocks are inappropriate (often SVT misdiagnosed as VT/VF).
📌 Indications
- Primary prevention:
- Ischaemic cardiomyopathy with LVEF ≤35% + inducible VT.
- Post-MI with LVEF ≤30% (MADIT II trial).
- Inherited syndromes: long QT, HCM, Brugada, ARVC.
- Secondary prevention:
- Cardiac arrest due to VT/VF.
- Sustained VT with structural heart disease.
- Unexplained syncope + inducible VT/VF with structural heart disease.
- CRT Devices:
- CRT-D (resynchronisation + defibrillator) or CRT-P (pacing only).
- Used in HF with QRS ≥130 ms + LVEF ≤35% (NYHA II–IV).
🔍 Types
- Single-chamber ICD: RV lead only.
- Dual-chamber ICD: RA + RV leads.
- CRT-D: biventricular pacing + defibrillation.
- CRT-P: biventricular pacing only.
🧾 Follow-Up
- ICD clinic checks scar, device function, battery life.
- Follow-up: 1–3 months post-implant → then every 3–6 months.
- Battery replacement ~6–8 years (minor operation).
🚨 Shocks & Troubleshooting
- Shocks = red flag → assess patient + device.
- Inappropriate shocks → psychological distress; ↑ mortality risk.
- SVT/AF/VT with compromise → manage as usual (external DC shock, IV amiodarone, beta-blockers).
⚠️ Place pads AP (avoid pocket site).
- Repetitive inappropriate shocks → place magnet over ICD to inhibit shocks.
- Contact during shock is harmless (gloves reduce discomfort).
⛔ Deactivation
- Apply magnet over ICD bump (usually left chest under clavicle).
- Ensure patient not pacing-dependent before permanent deactivation.
📚 References
