
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Decompressive Hemicraniectomy
Related Subjects: |Neurological History taking |Causes of Stroke |Ischaemic Stroke |Subarachnoid Haemorrhage |Small Vessel Disease |Vascular Dementia |Capsular and Pontine Warning Syndromes |Dementias |CADASIL |CARASIL |Cerebral Arterial Perfusion and Clinical Correlates |Anterior circulation Brain |Posterior circulation Brain |Acute Stroke Assessment (ROSIER&NIHSS) |Carotid Artery dissection |Vertebral artery dissection |Acute Stroke Assessment (ROSIER&NIHSS) |Atrial Fibrillation |Atrial Myxoma |Causes of Stroke |Ischaemic Stroke |Cancer and Stroke |Cerebral Venous thrombosis |Cardioembolic stroke |CT Basics for Stroke |Endocarditis and Stroke |Haemorrhagic Stroke |Stroke Thrombolysis |Hyperacute Stroke Care |AP of the Brain |Cryptogenic stroke |Carotid Web |Anterior / Medial Medullary Infarct (Dejerine Syndrome)
Decompressive hemicraniectomy with durotomy, first performed by Harvey Cushing in 1905, was initially applied in trauma and infection but gained prominence in stroke care after 1956. It remains one of the most dramatic yet lifesaving neurosurgical interventions in malignant MCA infarction.
🧾 About
- Aimed at preventing death from malignant middle cerebral artery (MCA) infarction with space-occupying cerebral edema.
- The procedure removes a large bone flap (12–14 cm diameter), with dural expansion to allow the swollen brain to herniate outward rather than downward, avoiding fatal brainstem compression.
- Mortality reduction is significant, though most survivors have moderate-to-severe disability - hence, careful patient/family discussions are essential.
- Also applicable in selected cases of large intracerebral haemorrhage, venous sinus thrombosis with mass effect, or fulminant encephalitis.
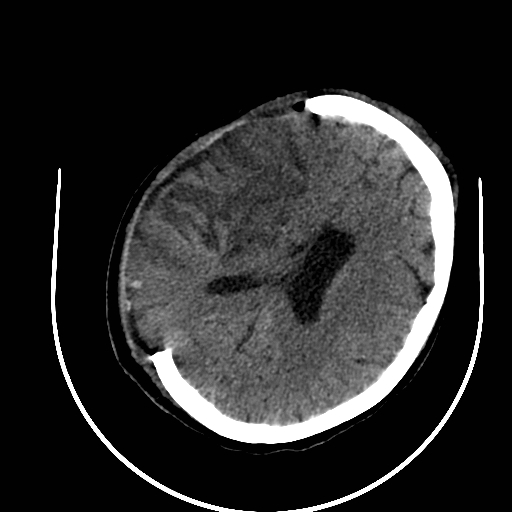
Right hemicraniectomy for R MCA infarct
📋 Current Selection Criteria
- Age ≤ 60 years (older patients may still be considered depending on functional baseline and wishes).
- Large MCA infarct (≥ 50% territory on CT or infarct volume >145 cm³ on DWI MRI).
- Clinical severity: NIHSS >15, reduced GCS/alertness (NIHSS 1a ≥1).
- Deterioration within 24–48 hours despite maximal medical therapy.
- Absence of severe pre-stroke disability (mRS ≤ 2 before the event).
📖 Pathophysiology Reminder
Malignant MCA infarction causes cytotoxic + vasogenic edema peaking at 3–5 days. Intracranial pressure rises, reducing cerebral perfusion and risking transtentorial herniation. Hemicraniectomy breaks the Monro–Kellie doctrine by removing the rigid skull barrier.
🇺🇸 AHA Guidelines (2018)
- Patients ≤ 60 years:
- Hemicraniectomy + durotomy reduces mortality by ~50%.
- ~55% survivors achieve mRS ≤ 3 (able to walk independently with or without aid).
- ~18% achieve mRS 2 (independent in daily life) at 12 months.
- Patients > 60 years:
- Mortality reduction ~50% still seen.
- Only ~11% reach mRS 3 (walk with help), virtually none achieve independence.
- Quality-of-life and ethical considerations are crucial - shared decision-making is essential.
- Adjunct therapies:
- Osmotic agents (mannitol, hypertonic saline) for cerebral edema.
- Short-term hyperventilation (Pco₂ 30–34 mmHg) as a bridge to definitive therapy.
- Corticosteroids are contraindicated - ineffective, ↑ risk of infection and GI bleeding.
🧑⚕️ Clinical Pearls
- Involves a large fronto-temporo-parietal bone flap - too small a craniectomy risks “mushrooming” and venous compression.
- Bone flap is stored in a subcutaneous abdominal pocket or freezer for later cranioplasty.
- Edema often peaks on day 3–5 post-infarct → anticipate deterioration even if initially stable.
- Outcomes vary: survival ≠ independence, so advance care planning is crucial.
📚 References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery