Related Subjects:
|Brain tumour s
|Astrocytomas
|Brain Metastases
|Tuberous sclerosis
|Turcot's syndrome
|Lhermitte Duclos Disease
|Oligodendroglioma
|Acute Hydrocephalus
|Intracranial Hypertension
|Primary CNS Lymphoma (PCNSL)
⚠️ Important: A normal CT or MRI does not exclude raised intracranial pressure (ICP).
Imaging is mainly used to detect mass effect, midline shift, obstructive hydrocephalus, herniation risk, or other structural causes.
In suspected idiopathic intracranial hypertension (IIH), diagnosis requires lumbar puncture (LP) with opening pressure measurement after appropriate neuroimaging has excluded a contraindication.
Never perform LP when there is suspicion of a lesion causing a pressure gradient across intracranial compartments, such as a large mass lesion, obstructive hydrocephalus, posterior fossa lesion, or established herniation → risk of catastrophic brain herniation.
📌 About
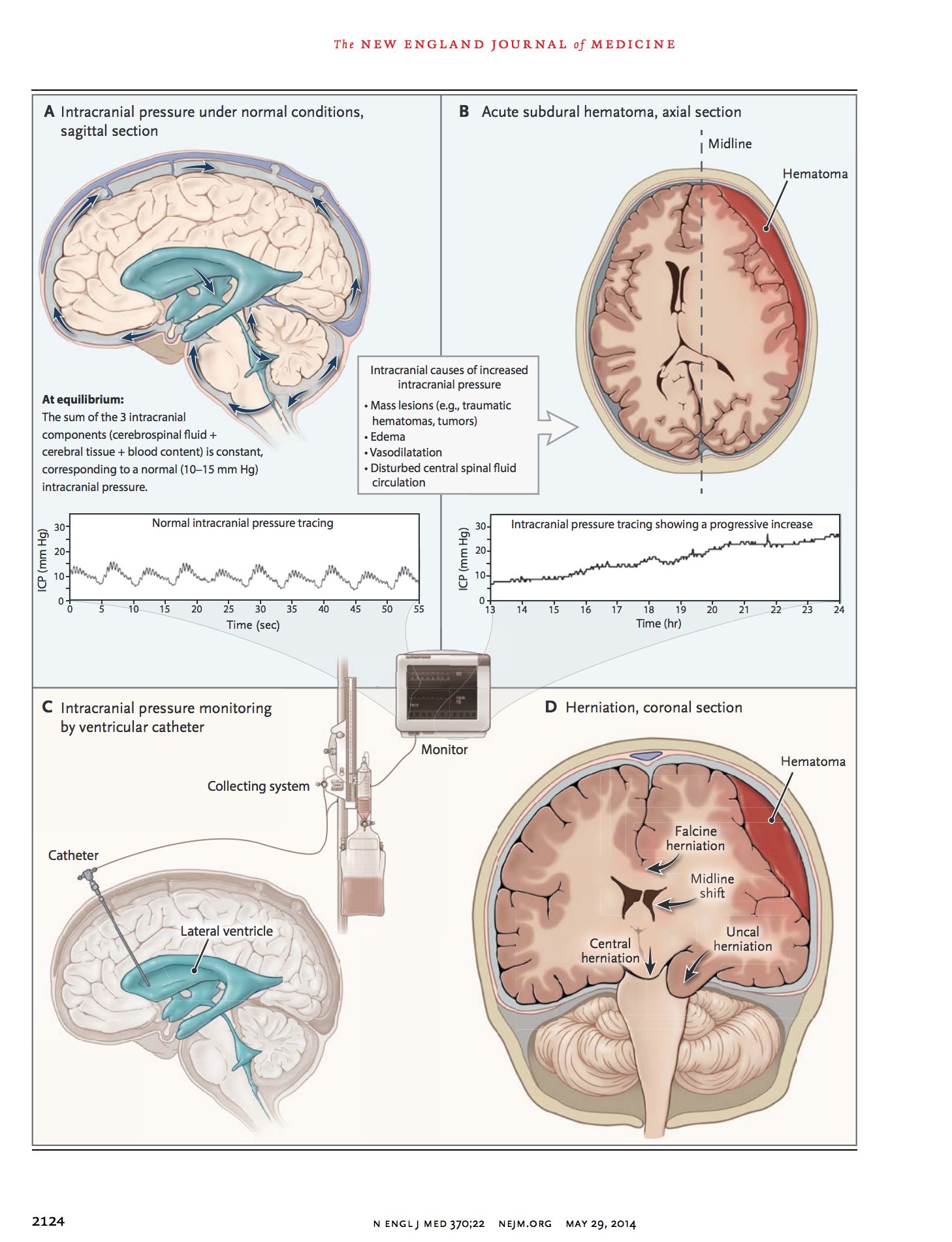
- The cranial vault contains brain tissue, blood, and CSF (Monro–Kellie doctrine). Because the skull is rigid, an increase in one compartment must be offset by a decrease in another, or ICP rises.
- CSF production is approximately 500 mL/day, mainly by the choroid plexus, with a total circulating CSF volume of roughly 150 mL.
- CSF is absorbed via arachnoid granulations into the dural venous sinuses; impaired absorption, obstructed flow, increased venous pressure, or an expanding intracranial lesion can all raise ICP.
- Raised ICP is a syndrome, not a diagnosis. The cause may be tumour, haemorrhage, oedema, hydrocephalus, venous sinus thrombosis, infection, or IIH.
- IIH is a diagnosis of exclusion: raised ICP with normal brain parenchyma on imaging, no mass lesion or hydrocephalus, and no alternative cause of intracranial hypertension identified.
🧠 Why LP Can Be Dangerous
- LP lowers pressure in the spinal CSF compartment.
- If there is a focal obstructing lesion or uneven intracranial pressure gradient, this can precipitate downward displacement of brain tissue.
- This may lead to transtentorial (uncal), central, or tonsillar herniation, causing coma, respiratory failure, or death.
- By contrast, in IIH there is typically diffusely elevated pressure without a mass lesion, so LP is often part of diagnosis and may transiently relieve symptoms.
🚫 When NOT to Perform LP
- Midline shift or radiological evidence of herniation.
- Large intracranial mass lesion with surrounding oedema (tumour, abscess, haematoma).
- Posterior fossa lesion causing crowding near the foramen magnum.
- Obstructive (non-communicating) hydrocephalus.
- Markedly reduced consciousness where a structural lesion has not yet been excluded.
- Clinical concern for a dangerous intracranial pressure gradient even if imaging is pending.
📷 When to Get Imaging Before LP
- Papilloedema.
- Focal neurological deficit (e.g. hemiparesis, aphasia, gaze palsy).
- Reduced or fluctuating consciousness.
- New-onset seizure or seizure in the current illness.
- Markedly progressive, severe, or unexplained headache.
- Signs of herniation: anisocoria, abnormal posturing, deteriorating GCS.
- Cushing response: hypertension with bradycardia ± irregular respirations (late sign).
- Suspicion of space-occupying lesion, hydrocephalus, or cerebral venous sinus thrombosis.
🧬 Aetiology of Raised ICP
- Mass lesions: primary brain tumour, metastasis, abscess.
- Haemorrhage: intracerebral, subdural, epidural, subarachnoid haemorrhage.
- Cerebral oedema: traumatic brain injury, malignant MCA infarction, encephalitis, hepatic failure, hypoxic injury.
- Hydrocephalus: obstructive (non-communicating) or communicating due to impaired absorption.
- Venous outflow obstruction: cerebral venous sinus thrombosis.
- Infection/inflammation: meningitis, encephalitis.
- Idiopathic intracranial hypertension: raised ICP without mass lesion or hydrocephalus.
- Other secondary causes of intracranial hypertension: some drugs (e.g. tetracyclines, vitamin A derivatives), endocrine/metabolic disorders, venous sinus stenosis.
👁️ Who Gets IIH?
- Most commonly affects women of childbearing age with obesity, but can occur in men, children, and people with lower BMI.
- Symptoms are driven by raised ICP and the major morbidity is visual loss.
- Secondary causes must be excluded, particularly cerebral venous sinus thrombosis and medication-related intracranial hypertension.
🔎 Clinical Features of Raised ICP
- Headache - often worse on waking, with coughing, straining, or lying flat.
- Nausea/vomiting - classically projectile, though this is not always present.
- Visual disturbance - transient visual obscurations, blurred vision, enlarged blind spot, diplopia.
- Papilloedema - important sign, but absence does not completely exclude raised ICP.
- VI nerve palsy - false localising sign causing horizontal diplopia.
- Declining conscious level, agitation, confusion, or reduced attention in more severe cases.
- Bradycardia, hypertension, irregular breathing - late pre-terminal signs.
- In infants: bulging fontanelle, separated sutures, increasing head circumference, “sunsetting” eyes.
🔎 Clinical Features Suggestive of IIH
- Daily or near-daily headache, often migraine-like.
- Transient visual obscurations lasting seconds.
- Pulsatile tinnitus (“whooshing” sound in time with the pulse).
- Horizontal diplopia from VI nerve palsy.
- Papilloedema on fundus examination.
- Visual field loss if disease is advanced or uncontrolled.
🧪 Investigations
- Urgent CT head if acute deterioration, focal deficit, trauma, or suspected haemorrhage/hydrocephalus.
- MRI brain is often better for posterior fossa lesions, subtle mass lesions, and features supportive of IIH.
- MRV or CTV if cerebral venous sinus thrombosis is suspected; this is especially important in presumed IIH.
- Ophthalmology assessment: visual acuity, colour vision, pupils, formal visual fields, optic disc assessment/OCT where available.
- LP opening pressure measured in the lateral decubitus position with legs relaxed, only after contraindications are excluded.
- CSF analysis if infection/inflammation is suspected and LP is safe to perform.
- Further imaging for malignancy if there is concern about metastatic disease or paraneoplastic process.
🧾 Imaging Findings That May Support IIH
- Imaging may be reported as normal.
- Possible supportive features include empty or partially empty sella, flattening of the posterior sclera, optic nerve sheath distension, and transverse sinus stenosis.
- These findings are supportive, not diagnostic, and their absence does not exclude IIH.
📏 Opening Pressure in LP
- Opening pressure should be interpreted in clinical context and alongside neuro-ophthalmic findings.
- In adults, an opening pressure of >25 cm CSF is commonly used to support IIH when the rest of the picture fits.
- The CSF composition in IIH should otherwise be normal.
⚠️ Complications
- Brain herniation → coma, respiratory arrest, death.
- Progressive visual loss from persistent papilloedema → optic atrophy and blindness.
- Hydrocephalus with acute neurological deterioration.
- Seizures depending on the underlying cause.
💊 Immediate Management of Suspected Raised ICP
- Urgent ABC assessment and senior/neurosurgical input where appropriate.
- Elevate head of bed to about 30° if not contraindicated.
- Avoid hypoxia, hypercapnia, hypotension, and fever.
- Treat the underlying cause urgently.
- For severe acute deterioration, neurocritical care measures may include airway protection, osmotherapy, and definitive neurosurgical intervention depending on cause.
💊 Cause-Specific Management
- Hydrocephalus: ventricular drainage, ventriculoperitoneal shunt, or endoscopic third ventriculostomy depending on cause.
- Brain tumour with oedema: dexamethasone, neurosurgical decompression/debulking, oncological treatment.
- Haematoma: urgent neurosurgical evacuation when indicated.
- Malignant MCA infarction: decompressive hemicraniectomy in selected patients.
- CVST: anticoagulation unless contraindicated, plus management of raised ICP and seizures where needed.
- Meningitis/encephalitis: urgent antimicrobial/antiviral treatment; do not delay therapy unnecessarily while waiting for imaging if CNS infection is strongly suspected.
- IIH: weight reduction, acetazolamide, headache management, and urgent surgical options (e.g. CSF diversion or optic nerve sheath fenestration) if vision is threatened.
👁️ Vision-Threatening IIH
- Rapidly worsening visual fields or acuity is an emergency.
- These patients need urgent specialist input because the priority is preserving vision, not simply treating headache.
- Repeated LPs are generally not definitive long-term management.
📝 Practical Exam / Ward Round Pearls
- Raised ICP is not the same as “do not LP”. The real issue is whether there is a pressure gradient caused by a structural lesion or obstruction.
- IIH is the classic exception: pressure is raised, but LP is part of diagnosis once imaging has excluded a dangerous cause.
- Papilloedema means think carefully: image first, assess vision, and consider MRV/CTV.
- A normal scan does not “rule out” raised ICP; it may simply rule out the dangerous causes that make LP unsafe.
📚 References