Hyperprolactinaemia
Related Subjects:
|Male Infertility
|Prolactin
|Prolactinoma
|Hyperprolactinaemia
|Sheehan's syndrome
|Acromegaly and Giantism
🍼 Raised Prolactin – Clinical Effects
- Galactorrhoea: seen in up to 90% of women, but <10% of men.
- 🌡️ Hypogonadotropic hypogonadism: Prolactin suppresses hypothalamic GnRH release → ↓ LH/FSH → menstrual irregularities, infertility, erectile dysfunction.
- 🦴 Long-term hyperprolactinaemia is linked to low bone mineral density (osteopenia/osteoporosis).
- ❤️ Reduced libido independent of gonadal status.
- 🤯 May cause headaches or visual disturbance if due to macroadenoma (mass effect).
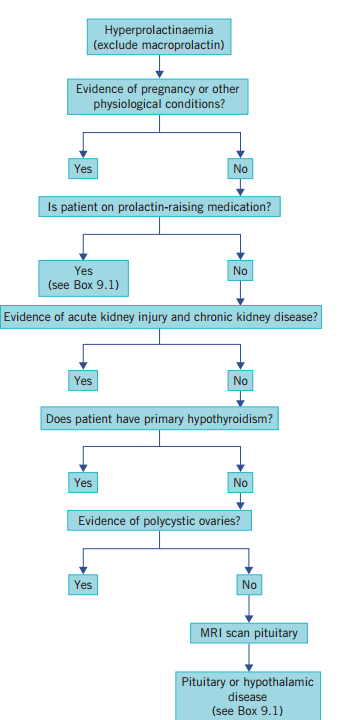
🔎 Causes of Raised Prolactin
- 🎯 Pituitary adenoma (Prolactinoma) → usually very high prolactin levels (>3000 mU/L).
- Physiological: Pregnancy, breastfeeding, nipple stimulation, chest wall trauma.
- Systemic: Stress, seizures, chronic kidney disease, cirrhosis, hypothyroidism.
- Drugs 💊:
- Dopamine antagonists: Antiemetics (metoclopramide, domperidone)
- Antipsychotics (risperidone, haloperidol),
- Some antidepressants.
- Opiates, antiretrovirals, cocaine.
- Structural: Stalk compression (loss of tonic dopamine inhibition).
- Granulomatous disease: Sarcoidosis, hypothalamic infiltration.
📏 Normal Values
- Serum prolactin: < 20 ng/mL (≈ < 400 mU/L)
- Note: Mild elevations (500–1000 mU/L) often drug-related; marked elevations (>3000 mU/L) suggest prolactinoma.
🧪 Key Investigations
- Serum prolactin (repeat to confirm; avoid stress during sampling).
- TFTs (exclude hypothyroidism).
- Renal and liver function tests.
- Pituitary MRI if prolactin markedly elevated or symptoms of mass effect.
💊 Management (Overview)
- First-line: Dopamine agonists (Cabergoline, Bromocriptine) → shrink adenoma + normalise prolactin.
- Treat underlying causes (e.g., hypothyroidism, drug withdrawal if possible).
- Trans-sphenoidal surgery if resistant/intolerant to medical therapy or with visual field compromise.
- Bone density monitoring due to risk of osteoporosis.