
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Right Ventricular Outflow Tract Tachycardia (RVOT)
Related Subjects: |Classical Ventricular Tachycardia |Idiopathic Ventricular Tachycardia |Right Ventricular Outflow Tract Tachycardia |Idiopathic Fascicular Left Ventricular Tachycardia |Left Ventricular Outflow Tract Tachycardia |Ventricular Fibrillation |Resuscitation - Adult Tachycardia Algorithm |Resuscitation - Advanced Life Support |Automatic Implantable Cardioverter Defibrillator (AICD)
⚡ Idiopathic ventricular tachycardia (IVT) in patients with an anatomically normal heart is a distinct entity. Its management and prognosis differ from VT associated with structural heart disease. 👉 RVOT VT is the commonest form of idiopathic VT, and should always be distinguished from ARVC/ARVD.
📖 About
- A form of Idiopathic Ventricular Tachycardia (IVT).
- ~80% of IVT cases arise from the Right Ventricular Outflow Tract (RVOT). 🫀
- ECG: Typically shows LBBB morphology because the arrhythmia originates in the RV. 📉
🧬 Aetiology & Mechanism
- Occurs in the absence of structural heart disease ✅.
- Usually due to a re-entrant or triggered activity mechanism involving the RVOT.
- Classically non-sustained, repetitive, and monomorphic VT.
- Triggered by exercise, stress, or catecholamine surges (adrenergic-dependent). 🏃♀️💉
✅ Diagnostic Criteria
- No structural heart disease (confirmed by Echo/CMR).
- No metabolic or electrolyte abnormalities (exclude hypokalaemia, hypomagnesaemia, thyroid). 🔬
- No inherited channelopathy (e.g., Long QT, Brugada, CPVT).
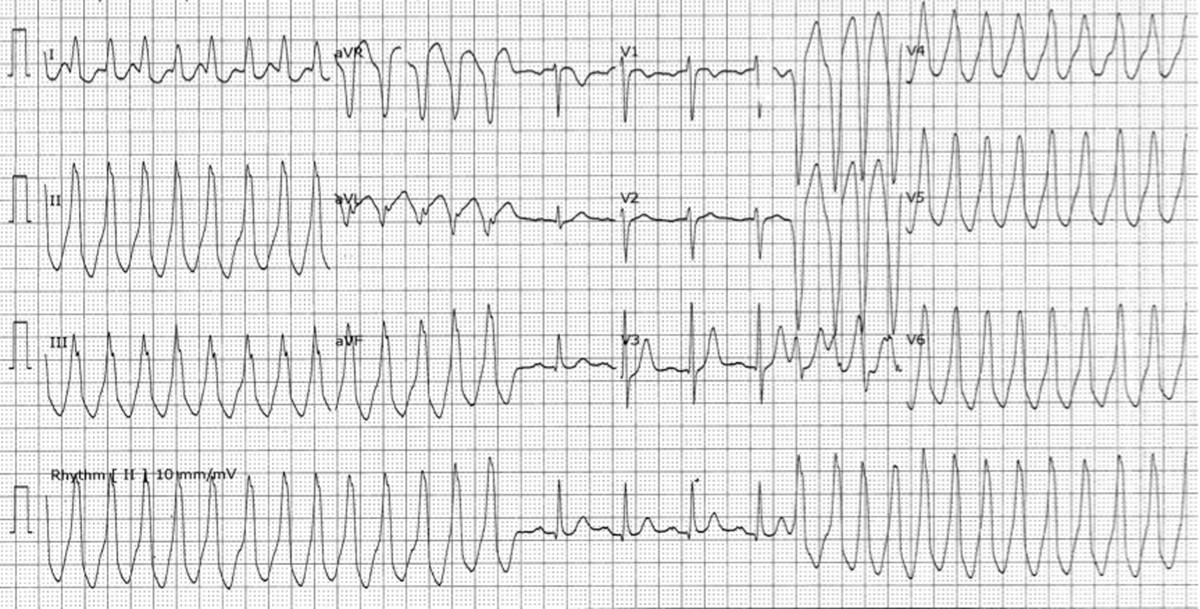
📊 RVOT VT ECG Example
👩⚕️ Clinical Features
- Commoner in females, typically aged 30–50 years 👩.
- Paroxysmal, exercise-induced sustained VT episodes. 🏋️♀️
- Symptoms: Palpitations 💓, presyncope/syncope 😵, occasional chest tightness.
- Often well tolerated but recurrent → lifestyle impairment.
🧪 Investigations
- 🧾 Bloods, Echo, CXR: Normal.
- 📉 ECG during VT: LBBB morphology + inferior axis (due to RVOT origin). → rS in V1 and tall R in V6 are typical. 👉 Key exam pearl: ARVD/ARVC differs - resting ECG often shows T-wave inversion in V1–V3 ± epsilon wave.
- 🏃♀️ Exercise stress test: May provoke VT (adrenergic trigger).
- 🧲 MRI: Can show subtle RV wall abnormalities in up to 70% (but be cautious - overlaps with ARVD).
🚨 Classical VT is still the most common cause of wide-complex tachycardia. There is no completely reliable way to distinguish classical VT from idiopathic VT or SVT with aberrancy by surface ECG alone. 👉 Always treat as VT until proven otherwise.
💊 Management
- 🔑 First rule: If diagnosis not certain ➝ treat as classical VT per ALS Adult Tachycardia algorithm.
- ABC + early Echo to confirm LV function.
- 🏥 If stable RVOT VT confirmed ➝ may terminate with Adenosine 6–24 mg (diagnostic & therapeutic). ❗ Not effective in ARVD.
- Verapamil IV (10 mg over 3–5 min) can be effective, but only if Echo confirms normal LV function. ⚡ Be prepared for DC cardioversion if patient deteriorates.
- Beta-blockers (especially non-selective) may suppress adrenergic-triggered VT.
- 💡 Radiofrequency ablation (RF ablation) offers curative treatment with >85–90% success rates for recurrent symptomatic RVOT VT.
📚 References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery