Epistaxis
💡 The nasal blood supply lies very superficially, designed to humidify & warm inspired air - but at the cost of vulnerability to bleeding.
⚠️ Never underestimate epistaxis: patients can lose significant volumes (including occult blood if swallowed).
📖 About
- Epistaxis = bleeding from nasal mucosal vessels.
- Usually mild/self-limiting, but occasionally life-threatening.
- Blood may be swallowed → occult loss; always assess haemodynamic compromise (tachycardia, postural hypotension).
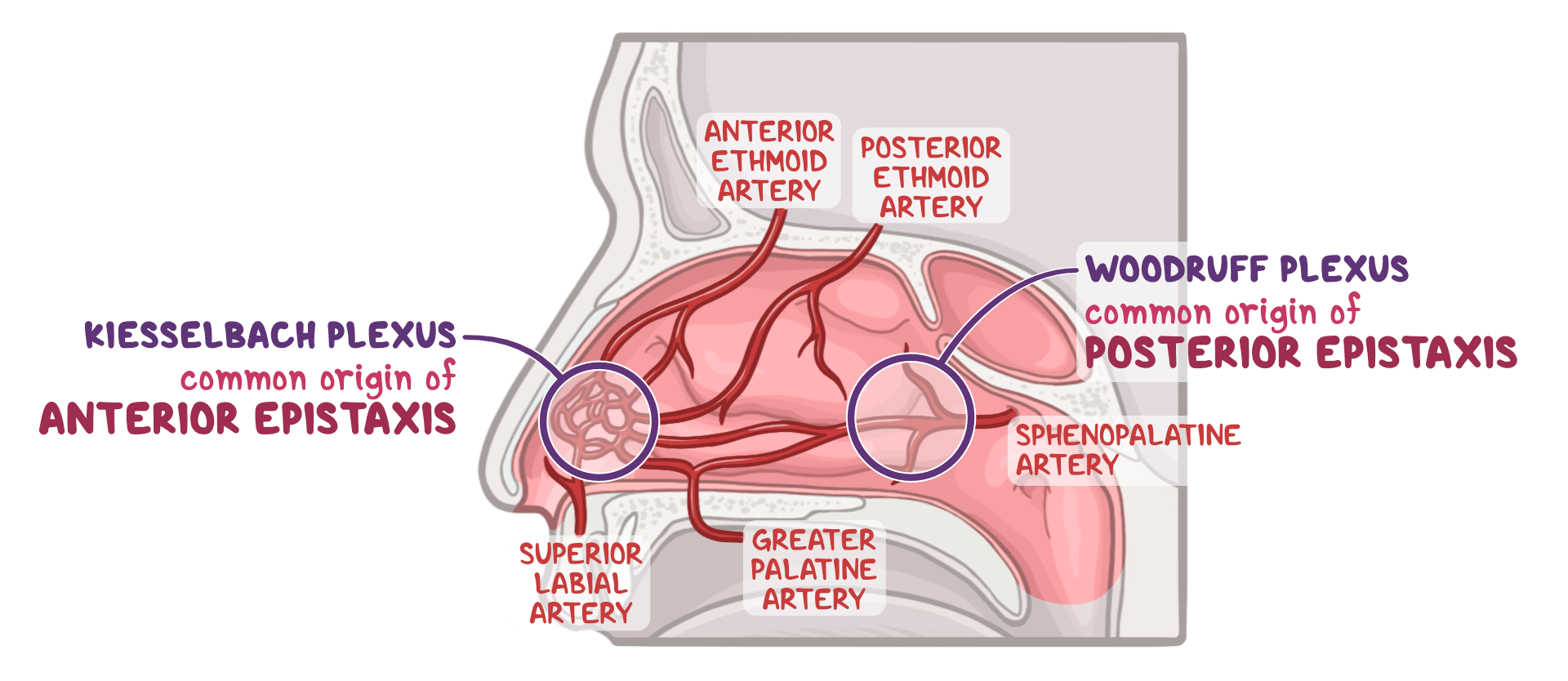
🧠 Anatomy
- ~90% arise from Kiesselbach’s plexus (Little’s area, anterior).
- Posterior bleeds = Woodruff’s plexus / sphenopalatine artery → severe, elderly, harder to control.
🩸 Risk Factors
- Hypertension, bleeding disorders, anticoagulants.
- Nasal trauma, nose-picking, recent URTI.
- Cocaine use, alcohol excess.
- Atherosclerosis, raised venous pressure (mitral stenosis).
- Haematological disease: thrombocytopenia, leukaemia, haemophilia.
🩺 Clinical Assessment
- History: duration, volume, triggers, family bleeding history.
- Drugs: warfarin, aspirin, clopidogrel, NSAIDs.
- Exam: anterior vs posterior, ENT look for masses/trauma.
🔎 Investigations
- FBC, U&E, clotting screen if coagulopathy suspected.
- Group & Save / X-match if severe bleeding.
⚠️ Complications
- Hypovolaemia, anaemia, shock.
- Packing complications (pressure necrosis, infection).
🛠️ Management
- Resus (ABC): IV access, monitoring, fluids/blood if needed.
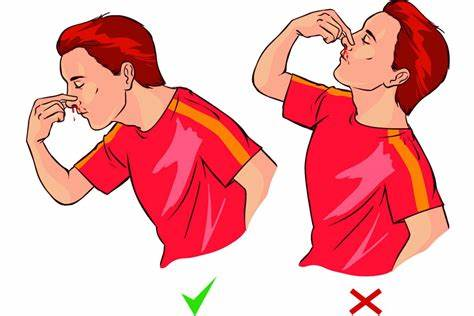
- First aid: Sit forward, pinch soft part of nose 10–15 mins, spit blood out (avoid swallowing).
- Topical: Clear clot, apply pledget with lidocaine + adrenaline.
- Cautery: Silver nitrate if visible anterior point (⚠️ only one side to avoid septal perforation).
- Packing: Merocel® / RapidRhino® if cautery fails or posterior bleed suspected → admit ENT.
- Posterior bleeds: Balloon/Foley catheter pack, antibiotics cover, ENT admission.
- Post-bleed advice: Avoid nose-blowing, hot drinks, alcohol, heavy lifting x 24 hrs.
🩺 Nasal Cautery Tips
- Clear clots, apply topical anaesthetic + vasoconstrictor.
- Identify bleeding point (red dot) → touch with silver nitrate 3–10 sec until grey-white.
- Apply Naseptin® cream after cautery.
👶 Children
- Most bleeds are anterior and minor, often from nose-picking or URTI crusting.
- Encourage simple first aid (pinch nose, lean forward).
- Cautery may be difficult; consider referral if recurrent or severe.
- Check for bleeding disorders (esp. if frequent/refractory).
- Reassure parents: most are self-limiting; use emollients (Vaseline) to keep mucosa moist.
🧓 Elderly
- More likely to have posterior bleeds (harder to control, greater blood loss).
- Often on anticoagulants or antiplatelets → check INR/medication history.
- Higher risk of hypovolaemia, anaemia, aspiration → admit if frail or recurrent.
- Consider hypertension and atherosclerosis as contributory factors.
- Posterior packing/IR embolisation may be required more frequently than in younger patients.
📌 Exam Pearls
- Anterior bleed → Little’s area (easy to compress). Posterior bleed → profuse, elderly, more serious.
- Always check anticoagulant history.
- Do not cauterise both septal sides (risk perforation).
- Persistent/recurrent epistaxis → exclude hypertension, coagulopathy, or tumour (esp. JNA in young males).
📖 References
