
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Aspergillus fumigatus
🦠 About
- Caused by spores of Aspergillus fumigatus seeding in a pre-existing lung cavity, often after prior lung damage.
- 📸 CXR: Apical opacity, partly opaque with a characteristic crescent sign or halo sign.
🔎 Aetiology
- Most common after tuberculosis (TB) cavitation.
- Lung cavities in fibrotic apices allow fungal colonisation.
- Aspergillus fumigatus isolated in up to 60% of patients with apical cavities.
- Other risks: COPD, sarcoidosis, prior cavitary infections.
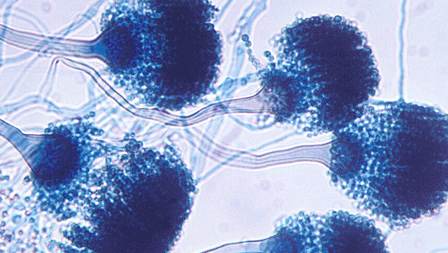
🧬 Characteristics
- Monomorphic filamentous fungus with acute-angle (<45°) branching hyphae.
- Ubiquitous in soil, damp environments, and decaying organic matter.
🩺 Clinical Manifestations
- 🤧 Allergic bronchopulmonary aspergillosis (ABPA)
- Occurs in asthmatics or those with allergies.
- High IgE, worsening asthma, recurrent infiltrates.
- Can cause progressive lung damage if untreated.
- ⚪ Aspergilloma (“fungus ball”)
- Forms within old lung cavities.
- Symptoms: chronic cough, hemoptysis, raised IgE.
- May remain silent but risk of massive bleeding.
- ⚡ Invasive aspergillosis
- Seen in immunosuppressed (transplant, chemo, prolonged steroids).
- Rapid progression → fever, chest pain, pulmonary infiltrates, systemic infection.
🧪 Investigations
- 📷 CXR & HRCT: Cavities, “fungus ball,” halo sign.
- Serum IgE (↑ in ABPA and aspergilloma).
- Sputum microscopy/culture (exclude TB).
- Galactomannan antigen & PCR → invasive disease.
💊 Management
- ✂️ Surgical resection: Considered for patients with symptomatic aspergilloma, especially when recurrent or massive hemoptysis threatens life.
- 🩸 Bronchial artery embolization: A potentially life-saving temporizing measure for massive hemoptysis; however, recurrence is common unless surgery follows.
- 💊 Itraconazole: Effective in ABPA (Allergic Bronchopulmonary Aspergillosis) and some cases of chronic pulmonary aspergillosis; reduces fungal burden and steroid requirement.
- ⭐ Voriconazole: First-line for invasive aspergillosis. May be combined with echinocandins (e.g. caspofungin) in severe or refractory disease.
- 💉 Amphotericin B: Reserved for resistant cases or when azoles are contraindicated; lipid formulations reduce nephrotoxicity risk.
- 🫁 Supportive care: Oxygen, ventilation, ITU support in invasive disease; optimize underlying lung disease (e.g. asthma, cystic fibrosis, COPD).
- 📉 Immunosuppression reduction: Critical in invasive disease where feasible (e.g. reduce steroids, adjust chemotherapy, review transplant immunosuppression).
📊 Quick Comparison: Aspergillus Syndromes
| Condition | Key Features | Management Highlights |
|---|---|---|
| 🤧 ABPA
(Allergic bronchopulmonary aspergillosis) |
|
|
| ⚪ Aspergilloma
(“fungus ball”) |
|
|
| ⚡ Invasive Aspergillosis |
|
|
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery