
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Penicillin Allergy
🧪 Penicillin allergy is often reported but rarely true: Around 10% of patients claim an allergy, yet <1% are truly allergic. Mislabeling leads to use of broader-spectrum, more toxic, and more expensive antibiotics, increasing risks of antimicrobial resistance and Clostridioides difficile infection.
- 🤔 Many “allergies” are side effects (e.g., nausea, vomiting) or viral rashes (e.g., amoxicillin + EBV infection) - not true allergies.
- ⌛ Sensitivity wanes: 50% lose penicillin allergy in 5 years, 80% in 10 years.
- 👶 Childhood penicillin “allergy” rarely persists into adulthood.
- 🔄 Cross-reactivity with cephalosporins is low (1–2%); most patients tolerate them.
- 🧪 Patients with mild, delayed reactions >10 years ago may be candidates for oral rechallenge under supervision.
- ✅ Careful assessment can often safely remove the penicillin allergy label.
- 💊 β-lactam allergies are the most common immune-mediated drug reactions encountered in clinical practice.
Taking a History of Penicillin Allergy
When a patient reports penicillin allergy, key questions include:
- 📜 Previous Reactions: Which antibiotics caused problems?
- 💊 Tolerated Antibiotics: Any β-lactams tolerated since?
- 🕒 Timing: How long ago did the reaction occur?
- ⚠️ Nature of Reaction: Was it diarrhoea, rash, swelling, breathing difficulty?
- 🎨 Rash Details: What type (maculopapular, urticarial, bullous)? Could it have been viral?
- ⏳ Onset: Minutes/hours (immediate IgE-mediated) vs days (delayed).
- 📍 Reason for antibiotic: Was it for a throat infection, skin infection, etc.?
- 🏥 Severity: Did it need hospitalisation or ICU?
- ✅ Resolution: Did it stop once the drug was discontinued?
- 📚 Sources: Ask patient, carers, GP, and check records.
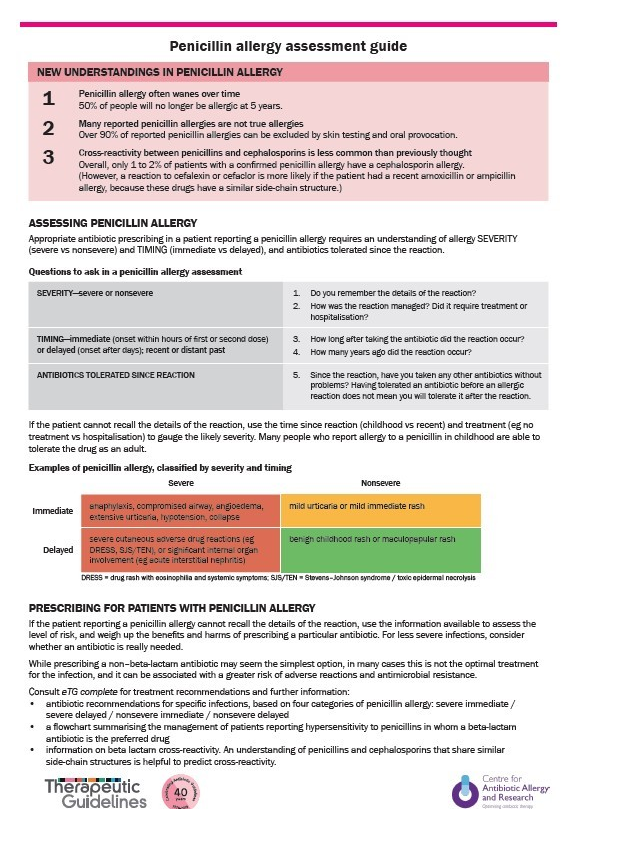
Risk Stratification
- 🚨 Immediate reactions (minutes–hours, IgE-mediated): urticaria, angioedema, bronchospasm, hypotension, anaphylaxis.
- 📆 Delayed reactions (days–weeks, T-cell mediated): morbilliform rash, serum sickness, Stevens-Johnson syndrome.
- 🔑 Differentiation matters: delayed mild rashes often allow safe future use under supervision.
📝 Exam pearl: Only 1 in 10 patients labelled as penicillin allergic are truly allergic. Always clarify the history before defaulting to alternatives.
Assessment and Management
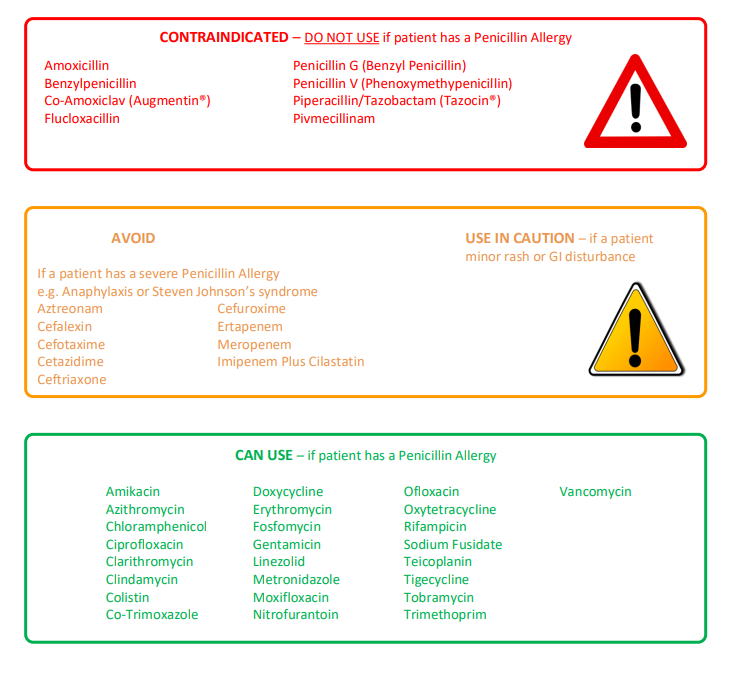
Understanding β-lactam classification helps guide safe prescribing:
- 🔴 Penicillins: Avoid in true allergy.
- 🟠 Other β-lactams (cephalosporins, carbapenems): Usually tolerated in mild allergy; caution in severe IgE-mediated cases.
- 🟢 Non-β-lactams: Always safe regardless of allergy history.
🌟 Delabelling strategies: Allergy testing (skin/IgE) and supervised oral challenge can safely remove false penicillin allergy labels, improving antibiotic stewardship.
Clinical Consequences of a False Allergy Label
- 💷 More expensive antibiotic prescriptions
- 🦠 Broader-spectrum antibiotics → antimicrobial resistance
- ⚠️ Higher rates of C. difficile infection
- ⏱️ Longer hospital stays & higher complication rates
References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery