
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
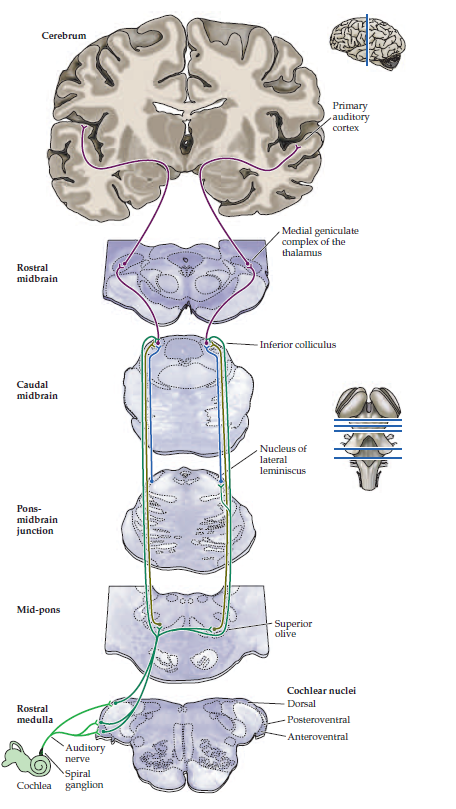
Assessing Hearing Loss
Related Subjects: |Assessing Hearing Loss |Benign Paroxysmal Positional Vertigo (BPPV) |Cholesteatoma |Epistaxis (Nosebleeds) |Acute Mastoiditis |Nasal polyps |Acute Sinusitis |Sudden Sensorineural Hearing loss (SNHL) |Causes of Vertigo |Tympanic (Eardrum) membrane perforation
⚠️ Urgent referral of hearing loss is required if it develops suddenly, is associated with Bell’s palsy, immunosuppression, or suspected stroke.
🛏️ Bedside Assessment
- Check comprehension and speech - dysphasia may confound assessment.
- Whisper test: whisper numbers in one ear while masking the other with finger rubbing.
- If unilateral loss detected → use Rinne and Weber to distinguish conductive vs sensorineural causes.
🧾 Key History Points
- Rapid onset (<3 days) = red flag → urgent ENT referral.
- Laterality: one or both ears affected?
- Associated symptoms: pain, discharge, tinnitus, vertigo, neurological symptoms (facial weakness, diplopia).
- Medication history: ototoxic drugs (aminoglycosides, loop diuretics, chemotherapy agents).
- Past/family history: hearing loss, noise exposure.
- Risk factors: immunosuppression, recent infections.
🔎 Examination
- Inspect outer ear, canal, and tympanic membrane.
- Look for discharge, swelling, perforation, cholesteatoma features.
- Check cranial nerves (esp. facial nerve palsy).
📏 Rinne & Weber Tests
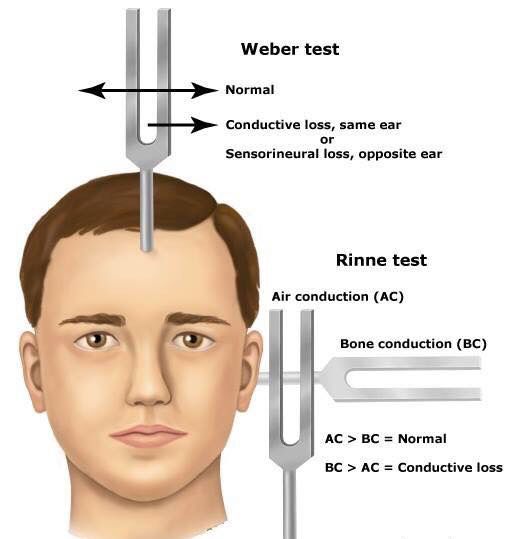
- Weber: – Conductive → sound localises to affected ear. – Sensorineural → sound localises to unaffected ear.
- Rinne: – Normal & sensorineural loss → AC > BC. – Conductive loss → BC > AC.
🧬 Causes of Hearing Loss
- Conductive: Wax, otitis externa/media, otosclerosis, barotrauma, perforated TM, local tumours.
- Sensorineural: Presbyacusis, noise-induced, Meniere’s, congenital, ototoxic drugs, acoustic neuroma, autoimmune inner ear disease.
🚨 Referral Criteria
- Immediate (<24h):
- Sudden hearing loss (≤30 days, developing in ≤3 days).
- Unilateral loss with facial droop or neurological features → urgent ENT / stroke pathway.
- Immunocompromised + hearing loss + otalgia/otorrhoea not improving within 72h.
- Urgent (within 2 weeks):
- Sudden loss developing over 3 days but >30 days ago.
- Rapidly progressive loss over 4–90 days.
- Adults of Chinese or SE Asian origin with unexplained middle ear effusion (ENT rule out nasopharyngeal carcinoma).
- Unexplained cases with: unilateral/asymmetric loss, fluctuating loss, hyperacusis, persistent distressing/pulsatile tinnitus, recurrent vertigo, or non-age-related loss.
📚 Reference
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery