
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
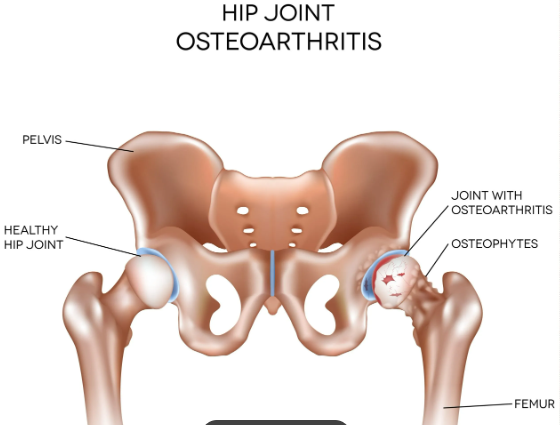
Hip Osteoarthritis ✅
Related Subjects: |Monoarticular arthritis |Polyarticular arthritis |Rheumatoid arthritis |Gout |Pseudogout |Septic Arthritis |Systemic Lupus Erythematosus (SLE) |Enteropathic Spondyloarthritis |Reactive Arthritis |Hip Osteoarthritis |Oxford Hip Score
🦴 Hip osteoarthritis is a common degenerative joint condition causing hip pain, stiffness and reduced function. It occurs when articular cartilage, subchondral bone and synovium become abnormal, leading to pain sensitisation, reduced movement and progressive disability.
📖 Overview
- Definition: OA is a clinical syndrome of joint pain with varying degrees of functional limitation and reduced quality of life.
- Hip OA: commonly causes groin pain, buttock pain, thigh pain or referred knee pain.
- Typical pattern: pain worsens with activity and improves with rest, although advanced disease may cause night pain or pain at rest.
- Diagnosis: usually clinical in adults aged over 45 with activity-related joint pain and either no morning stiffness or morning stiffness lasting less than 30 minutes.
⚠️ Risk Factors
- Increasing age
- Previous hip injury or fracture
- Developmental dysplasia of the hip
- Femoroacetabular impingement
- Obesity or increased joint loading
- Family history of osteoarthritis
- Inflammatory arthritis or avascular necrosis as alternative/secondary causes
- Occupational or sporting repetitive joint stress
🔍 Symptoms
- Groin pain, often worse on walking, stairs or standing from a chair
- Pain radiating to the buttock, lateral hip, thigh or knee
- Reduced walking distance
- Difficulty putting on socks, shoes or cutting toenails
- Stiffness after rest, usually brief
- Night pain in more advanced disease
- Reduced function, falls risk and loss of independence
🩺 Examination
- Antalgic gait or reduced stride length
- Reduced internal rotation is often an early sign
- Pain on hip flexion, internal rotation or abduction
- Reduced range of movement
- Trendelenburg gait if hip abductor weakness is present
- Assess lumbar spine, knees and neurovascular status if symptoms are atypical

🧪 Investigations
- Many cases can be diagnosed clinically without routine imaging.
- X-ray pelvis/hip is useful if diagnosis is uncertain, symptoms are atypical, severe symptoms are present, or referral for surgery is being considered.
- X-ray features include joint space narrowing, osteophytes, subchondral sclerosis and cysts.
- Blood tests are not routinely needed unless inflammatory arthritis, infection, malignancy or another diagnosis is suspected.
⚠️ Red flags: acute inability to weight-bear, fever, severe night pain, unexplained weight loss, history of cancer, trauma, rapidly worsening pain, suspected septic arthritis, fracture or avascular necrosis.
💪 Core Management
- Education: explain OA as a treatable long-term condition rather than simply “wear and tear”.
- Exercise: offer tailored therapeutic exercise, including strengthening and aerobic activity.
- Weight management: support weight loss if overweight or obese, as this can reduce pain and improve function.
- Activity pacing: encourage regular activity while avoiding repeated flare-provoking overload.
- Physiotherapy: useful for strengthening, range of movement, gait and function.
- Walking aids: a stick in the opposite hand can reduce hip joint load.
💊 Pain Management
- Topical NSAID: may be tried, although benefit for deep hip pain may be limited compared with knee/hand OA.
- Oral NSAID: consider if suitable, using the lowest effective dose for the shortest time.
- Gastroprotection: offer a proton pump inhibitor with oral NSAIDs where appropriate.
- Paracetamol: may be used by some patients, but should not be relied on as the main long-term treatment if ineffective.
- Opioids: avoid routine long-term use because benefits are limited and harms include falls, constipation, sedation and dependence.
- Intra-articular corticosteroid injection: may provide short-term relief in selected patients, especially to support exercise or manage a flare.
🏥 When to Refer
- Persistent pain, stiffness and reduced function despite optimal non-surgical management.
- Symptoms substantially affect quality of life, sleep, mobility, work or independence.
- Marked restriction in activities of daily living.
- Diagnostic uncertainty or suspected alternative pathology.
- Consider orthopaedic referral for possible hip replacement when symptoms are refractory and significant.
✅ Referral for joint replacement should be based on symptoms, function, quality of life and patient preference. NICE advises that age, sex, smoking, comorbidities, obesity or BMI should not be used as barriers to referral for joint replacement assessment.
📊 Oxford Hip Score
- The Oxford Hip Score is a patient-reported questionnaire assessing hip pain and function.
- It is commonly used before and after hip replacement to monitor severity and outcome.
- It can help quantify how much hip symptoms affect daily activities.
- It should support, not replace, shared clinical decision-making.
🧠 Clinical Pearl
Hip osteoarthritis often presents as groin pain with reduced internal rotation, but pain may be referred to the knee, so always examine the hip in an older adult with unexplained knee pain. The pathology is not just “cartilage loss”: subchondral bone change, synovitis, osteophytes and pain sensitisation all contribute to symptoms. Management should focus on function, exercise and shared decision-making, with timely referral when quality of life is significantly affected.
📚 Exam Pearl
🦴 Hip OA = groin pain + reduced internal rotation + activity-related symptoms. First-line management is education, therapeutic exercise and weight support, with NSAIDs if suitable and referral for joint replacement assessment when symptoms remain severe despite conservative treatment.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery