
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Anatomy and Physiology of the Abdomen
Related Subjects: |Pulmonary Physiology |Pancreas Physiology |Renal Physiology |Pulmonary Physiology |Cardiac AP |Coronary AP |Cardiac Electrophysiology |Cardiac Embryology |Cardiac Physiology |Cardiac Physiology |Gastrointestinal tract Physiology |Autonomic Nervous System | Abdominal AP | Brainstem Anatomy | Thalamic Anatomy
The abdomen is the region of the body located between the thorax (chest) and the pelvis, housing many vital organs and structures involved in digestion, metabolism, excretion, reproduction, and other essential physiological processes. It is bounded superiorly by the diaphragm, which separates it from the thoracic cavity, inferiorly by the pelvic brim, posteriorly by the vertebral column and lumbar muscles, and laterally and anteriorly by the abdominal wall muscles. Understanding the anatomy and physiology of the abdomen is crucial for clinical examination, diagnosis, and treatment of various medical conditions, including gastrointestinal disorders, vascular diseases, and traumatic injuries.
Quadrants of the Abdomen
The abdomen is commonly divided into four quadrants by imaginary horizontal and vertical lines intersecting at the umbilicus, facilitating clinical assessment and localization of pain or pathology:
- Right Upper Quadrant (RUQ):
- Liver (right lobe, the largest lobe, responsible for detoxification, protein synthesis, and bile production)
- Gallbladder (stores and concentrates bile for fat digestion)
- Duodenum (first part of the small intestine, site of mixing with pancreatic enzymes and bile)
- Head of the pancreas (produces digestive enzymes and hormones like insulin)
- Right kidney and adrenal gland (kidney filters blood; adrenal produces hormones like cortisol and aldosterone)
- Part of the ascending and transverse colon (absorbs water and electrolytes)
- Right Lower Quadrant (RLQ):
- Cecum and appendix (appendix may play a role in gut immunity; inflammation leads to appendicitis)
- Ascending colon
- Right ovary and fallopian tube (in females; involved in reproduction)
- Right ureter (transports urine from kidney to bladder)
- Small intestine (ileum; absorbs nutrients like vitamin B12 and bile salts)
- Left Upper Quadrant (LUQ):
- Stomach (digests food via acid and enzymes)
- Spleen (filters blood, stores platelets, and supports immune function)
- Left lobe of the liver
- Body and tail of the pancreas
- Left kidney and adrenal gland
- Part of the transverse and descending colon
- Small intestine (jejunum; major site for nutrient absorption)
- Left Lower Quadrant (LLQ):
- Descending colon
- Sigmoid colon (S-shaped; stores feces before rectum)
- Left ovary and fallopian tube (in females)
- Left ureter
- Small intestine (ileum)
Regions of the Abdomen
For a more detailed assessment, the abdomen is also divided into nine regions by two horizontal lines (subcostal and intertubercular) and two vertical lines (midclavicular), allowing precise localization:
- Epigastric Region:
- Located above the umbilical region; contains the stomach, part of the liver, pancreas, and duodenum. Common site for epigastric pain from peptic ulcers or pancreatitis.
- Umbilical Region:
- Surrounds the umbilicus (navel); contains parts of the small intestine, transverse colon, and abdominal aorta. Often involved in umbilical hernias.
- Hypogastric (Suprapubic) Region:
- Located below the umbilical region; contains the bladder, sigmoid colon, and reproductive organs like the uterus in females. Pain here may indicate urinary tract infections or gynecological issues.
- Right Hypochondriac Region:
- Contains the liver (right lobe), gallbladder, and right kidney. Associated with conditions like cholelithiasis (gallstones).
- Left Hypochondriac Region:
- Contains the spleen, left kidney, and part of the stomach. Splenomegaly can be palpated here.
- Right Lumbar Region:
- Contains the ascending colon, part of the small intestine, and right kidney. Flank pain may suggest renal colic.
- Left Lumbar Region:
- Contains the descending colon and part of the small intestine.
- Right Iliac (Inguinal) Region:
- Contains the cecum, appendix, and part of the small intestine. Classic site for appendicitis pain (McBurney's point).
- Left Iliac (Inguinal) Region:
- Contains the sigmoid colon and part of the small intestine. Common for diverticulitis pain.
Muscles of the Abdomen
- Rectus Abdominis: Paired vertical muscles on either side of the midline (linea alba), divided by tendinous intersections into segments ("six-pack"); originates from pubic symphysis and inserts into xiphoid process and costal cartilages; responsible for flexing the trunk, compressing abdominal viscera, and maintaining posture and intra-abdominal pressure.
- External Oblique: Superficial lateral muscles originating from lower ribs and inserting into linea alba and iliac crest; fibers run inferomedially, assisting in trunk rotation (contralateral), lateral flexion, and compression of abdominal contents.
- Internal Oblique: Located beneath the external obliques, originating from iliac crest and thoracolumbar fascia, inserting into lower ribs and linea alba; fibers run superomedially, aiding in trunk rotation (ipsilateral), lateral flexion, and core stability.
- Transversus Abdominis: The deepest abdominal muscle, originating from iliac crest, thoracolumbar fascia, and lower ribs, inserting into linea alba; fibers run horizontally, acting like a corset to provide core stability, increase intra-abdominal pressure (e.g., during coughing or lifting), and compress abdominal contents.
These muscles form the anterior abdominal wall, supported by aponeuroses that converge at the linea alba. They are crucial for protecting organs, facilitating breathing, and enabling movements.
Vascular Supply
- Abdominal Aorta: Enters the abdomen through the aortic hiatus at T12, descends along the vertebral column, and bifurcates into common iliac arteries at L4; major blood vessel supplying the abdomen with oxygenated blood; branches include paired and unpaired vessels.
- Celiac Trunk: First major branch at T12; gives rise to the left gastric (supplies stomach), splenic (supplies spleen and pancreas), and common hepatic arteries (supplies liver, gallbladder, stomach, duodenum, and pancreas).
- Superior Mesenteric Artery: Arises at L1; supplies the small intestine (duodenum to mid-transverse colon), pancreas, and proximal large intestine via branches like jejunal, ileal, ileocolic, right colic, and middle colic arteries.
- Inferior Mesenteric Artery: Arises at L3; supplies the distal large intestine via left colic, sigmoid, and superior rectal arteries.
Venous drainage parallels arteries, ultimately into the portal vein (for gastrointestinal organs) or inferior vena cava. Anastomoses between superior and inferior systems provide collateral circulation.
Innervation
- The abdominal organs receive innervation from the autonomic nervous system, which regulates involuntary functions:
- Sympathetic Fibers: Arise from thoracic (T5-T12) and lumbar (L1-L2) spinal cord segments via splanchnic nerves; inhibit gastrointestinal motility and secretion, vasoconstrict blood vessels, and promote sphincter contraction during "fight or flight."
- Parasympathetic Fibers: Provided by the vagus nerve (cranial nerve X) for foregut and midgut, and pelvic splanchnic nerves (S2-S4) for hindgut; stimulate gastrointestinal motility, secretion, and relaxation of sphincters during "rest and digest."
- The celiac plexus (solar plexus) supplies sympathetic innervation to the foregut, while the superior mesenteric plexus supplies the midgut, and inferior mesenteric plexus the hindgut. Enteric nervous system (Meissner's and Auerbach's plexuses) provides local control.
- Somatic innervation to the abdominal wall comes from thoracoabdominal nerves (T7-T11), subcostal (T12), and iliohypogastric/ilioinguinal (L1) for sensation and motor function.
Omentum
- Definition: The omentum is a double-layered fold of peritoneum extending from the stomach to adjacent organs in the abdominal cavity, rich in fat and immune cells.
- Types:
- Greater Omentum:
- Extends from the greater curvature of the stomach, duodenum, and transverse colon, hanging over the intestines like an apron.
- Consists of four layers of peritoneum containing adipose tissue, blood vessels, lymphatics, and immune cells (macrophages and lymphocytes).
- Functions include fat storage for energy reserve, immune response by phagocytosing pathogens, protection of abdominal organs by isolating infections (e.g., sealing perforations), and limiting spread of inflammation.
- Lesser Omentum:
- Connects the lesser curvature of the stomach and the proximal duodenum to the porta hepatis of the liver.
- Divided into the hepatogastric ligament (stomach to liver) and hepatoduodenal ligament (duodenum to liver).
- Contains important structures, including the hepatic artery proper, portal vein, common bile duct (collectively the portal triad), lymphatics, and autonomic nerves.
- Greater Omentum:
- Clinical Significance:
- The greater omentum is often referred to as the "abdominal policeman" due to its role in immune responses and infection containment, migrating to sites of inflammation.
- Omental adhesions can occur after surgery or inflammation, potentially leading to complications like intestinal obstruction or chronic pain.
- Omental infarction, a rare condition where blood supply to a segment of omentum is compromised (e.g., due to torsion), can cause acute abdominal pain mimicking appendicitis and may require surgical intervention like omentectomy.
- In oncology, the omentum can be a site for metastatic spread (e.g., in ovarian cancer), and omentectomy is sometimes performed.
Peritoneum
- The peritoneum is a thin, serous membrane lining the abdominal cavity (parietal) and covering the abdominal organs (visceral), secreting fluid for lubrication.
- It consists of two main layers:
- Visceral Peritoneum:
- Covers the external surfaces of most abdominal organs, including the stomach, intestines, liver, spleen, and parts of the urogenital system.
- Provides lubrication via serous fluid to reduce friction between organs during movement (e.g., peristalsis).
- Contains blood vessels, lymphatics, and nerves supplying the abdominal organs; forms mesenteries suspending organs.
- Parietal Peritoneum:
- Lines the internal surface of the abdominal wall, extending from the diaphragm to the pelvic cavity.
- Supplies sensory innervation from spinal nerves, making it highly sensitive to pain, pressure, temperature, and chemical irritation (e.g., in peritonitis).
- Forms folds (ligaments and mesenteries) that anchor organs to the abdominal wall and contain blood vessels, nerves, and lymphatics.
- Visceral Peritoneum:
- Clinical Relevance:
- Peritonitis: Inflammation of the peritoneum, often due to bacterial infection (e.g., from perforated appendicitis or diverticulitis) or sterile causes (e.g., bile leak); presents with severe, diffuse abdominal pain, rigidity, and fever; requires immediate antibiotics and possibly surgery.
- Ascites: Pathological accumulation of fluid in the peritoneal cavity, resulting from portal hypertension (e.g., liver cirrhosis), heart failure, malignancy, or hypoalbuminemia; may necessitate diagnostic paracentesis for analysis and therapeutic drainage.
- Understanding the peritoneum's anatomy is crucial during surgical procedures like laparotomy to minimize complications, prevent adhesions, and ensure proper healing.
- The omentum and peritoneum play vital roles in the anatomy and function of the abdominal cavity, contributing to protection, support, immune defense, and organ mobility.
- A thorough understanding of these structures is essential for clinicians in diagnosing and managing abdominal conditions effectively, including differentiating visceral from parietal pain.
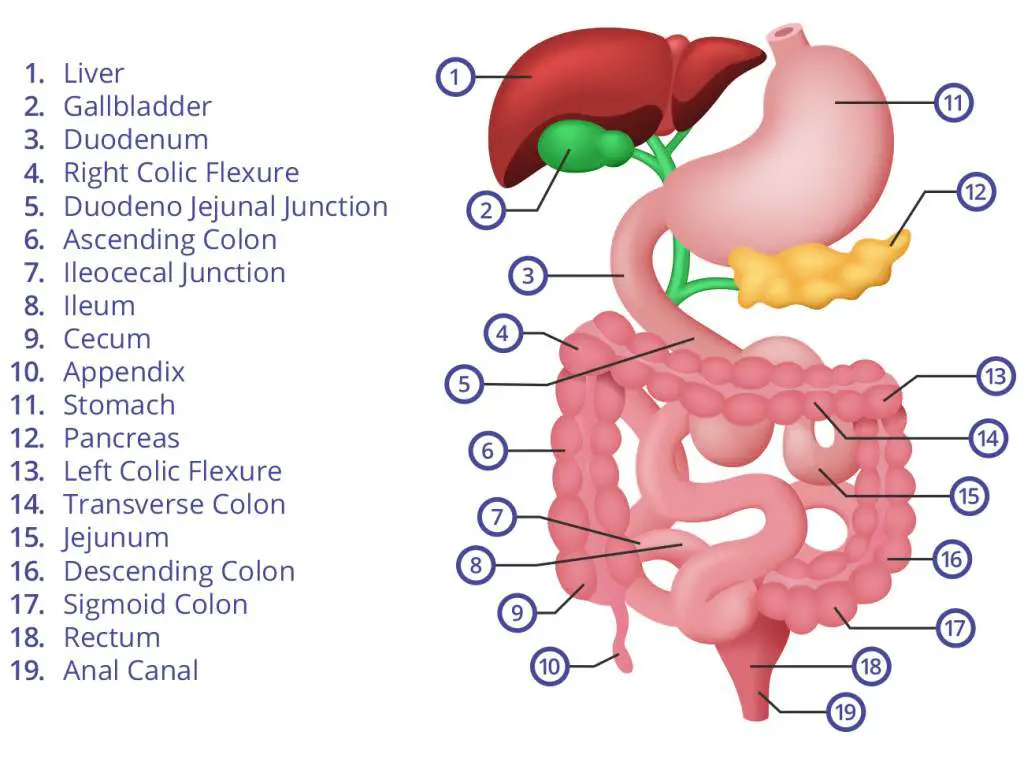
Gastrointestinal AP
Oesophagus
- Approximately 25 cm in length, connecting the pharynx to the stomach, passing through the neck, thorax, and diaphragm.
- Lined with non-keratinized stratified squamous epithelium to protect against abrasion from food boluses; transitions to columnar at the gastroesophageal junction.
- Muscular layers:
- Outer longitudinal muscle layer (shortens the esophagus during swallowing).
- Inner circular muscle layer (constricts to propel food).
- Muscle composition varies along its length:
- Upper third: Primarily striated (skeletal) muscle, under voluntary control via somatic nerves.
- Middle third: Mixture of striated and smooth muscle.
- Lower third: Primarily smooth muscle, under involuntary autonomic control.
- Protected from acid reflux by:
- Lower Oesophageal Sphincter (LES): A high-pressure zone (not anatomical sphincter) that relaxes during swallowing but maintains tone to prevent gastroesophageal reflux disease (GERD).
- Salivary and Oesophageal Bicarbonate Secretion: Neutralizes any acid that refluxes into the oesophagus via glands in submucosa.
- Gravity: Assists in keeping gastric contents in the stomach when in an upright position.
- "Pinchcock" Effect of Diaphragm: The right crus of the diaphragm encircles the esophagus, exerting external pressure to augment LES function, especially during inspiration.
- Peristalsis: Primary (initiated by swallowing) and secondary (triggered by distension) waves propel food; regulated by enteric nervous system and vagus nerve.
Stomach
- Located approximately 50 cm from the teeth along the digestive tract; J-shaped organ with capacity of 1-1.5 liters, expandable to 4 liters.
- Lined with simple columnar epithelium featuring rugae (folds) for expansion; the transition from squamous epithelium occurs at the oesophagogastric (OG) junction (Z-line).
- Secretes about 2–3 liters of gastric juices daily, with pH 1-3 for digestion.
- Gastric glands contain specialized cells:
- Parietal Cells: Secrete hydrochloric acid (HCl) via H+/K+ ATPase proton pumps and intrinsic factor essential for vitamin B12 absorption in the ileum; regulated by histamine, gastrin, and acetylcholine.
- Chief Cells: Produce pepsinogen, the inactive precursor of pepsin, which initiates protein digestion; also secrete gastric lipase for fat digestion.
- Surface Mucous Cells: Secrete mucus and bicarbonate (HCO3-) to form a protective barrier against acidic gastric juices and pepsin.
- Enteroendocrine Cells: Secrete hormones like gastrin (stimulates acid secretion) and somatostatin (inhibits).
- Innervation:
- Vagal Nerve (Parasympathetic): Provides motor and secretory signals via anterior and posterior trunks to stimulate digestion and motility.
- Meissner's (submucosal) and Auerbach's (myenteric) Plexuses (Enteric Nervous System): Coordinate local reflexes for secretion, blood flow, and gastric motility (mixing waves and peristalsis).
- Sympathetic Nervous System: From celiac plexus; inhibits digestive activity, decreases blood flow, and modulates pain.
- Phases of gastric secretion: Cephalic (sight/smell), gastric (food in stomach), intestinal (chyme in duodenum).
Small Intestine
- Approximately 6-7 meters in length in adults, divided into three sections with a surface area of ~200 m² due to plicae circulares, villi, and microvilli:
- Duodenum: ~25 cm, C-shaped around pancreas head; receives chyme from stomach via pyloric sphincter, pancreatic juice (enzymes like amylase, lipase, proteases) and bile (emulsifies fats) via major duodenal papilla; primary site for chemical digestion and iron/calcium absorption; retroperitoneal.
- Jejunum: ~2.5 m, in upper left abdomen; thick muscular wall, prominent plicae, and rich vascular supply for nutrient absorption (carbohydrates, proteins, fats, vitamins); intraperitoneal, suspended by mesentery.
- Ileum: ~3.5 m, in lower right abdomen; thinner wall, fewer plicae; absorbs vitamin B12 (via intrinsic factor), bile salts (recycled via enterohepatic circulation), and remaining nutrients; contains Peyer's patches (MALT) for immune surveillance against pathogens.
- Lined with simple columnar epithelium featuring villi (with lacteals for fat absorption) and microvilli (brush border with enzymes like disaccharidases, peptidases).
- Contains specialized structures:
- Crypts of Lieberkühn: Intestinal glands secreting succus entericus (intestinal juice) rich in enzymes, mucus, and enteropeptidase; house Paneth cells (antimicrobial) and stem cells for rapid epithelial renewal (every 3-5 days).
- Peyer's Patches: Aggregated lymphoid nodules in submucosa, especially ileum; sample antigens and initiate immune responses (IgA secretion).
- Functions:
- Completes digestion of macronutrients through pancreatic and brush border enzymes (e.g., maltase, lactase, enterokinase activates trypsinogen).
- Absorbs ~90% of nutrients, electrolytes, and water into bloodstream (via portal vein) or lymph (chylomicrons).
- Secretes hormones like cholecystokinin (CCK; stimulates gallbladder and pancreas), secretin (stimulates bicarbonate secretion), and motilin (regulates migrating motor complex).
- Motility regulated by:
- Segmental Contractions: Mix chyme with digestive juices, enhance contact with mucosa for absorption.
- Peristalsis: Propels contents aborally at 1-2 cm/sec; coordinated by enteric nervous system.
- Enteric Nervous System: Independent control via reflexes; modulated by autonomic input.
- Migrating motor complex (MMC) clears undigested material during fasting.
Large Intestine
- Approximately 1.5 meters in length, wider diameter than small intestine (~6 cm), comprising:
- Cecum: Blind pouch inferior to ileocecal valve; receives chyme from ileum; contains the vermiform appendix, a lymphoid organ involved in gut immunity and microbiome reservoir.
- Colon: Divided into ascending (right side, retroperitoneal), transverse (across abdomen, intraperitoneal), descending (left side, retroperitoneal), and sigmoid (S-shaped, intraperitoneal) sections; responsible for water (~1L/day) and electrolyte absorption, forming semisolid feces.
- Rectum and Anal Canal: Rectum (~15 cm) stores feces; anal canal (~4 cm) with internal (involuntary smooth muscle) and external (voluntary skeletal) sphincters for continence.
- Lined with simple columnar epithelium with numerous goblet cells for mucus; transitions to stratified squamous at anal canal for protection; no villi, but crypts for absorption and secretion.
- Functions:
- Absorbs remaining water, sodium, chloride, and potassium from indigestible residue.
- Forms, stores, and compacts feces via mucus lubrication and bacterial action.
- Hosts ~10^14 gut microbiota that ferment undigested carbohydrates (producing short-chain fatty acids for energy), synthesize vitamins (K, biotin, folate), and modulate immunity.
- Distinctive features:
- Haustra: Sacculations or pouch-like segments formed by incomplete circular muscle, aiding in mixing and water absorption.
- Taeniae Coli: Three longitudinal smooth muscle bands running the length of the colon; their tonic contraction creates haustra and facilitates propulsion.
- Epiploic Appendages: Small, fat-filled peritoneal pouches attached to the serosa; may serve as fat storage or cushioning, but can infarct causing pain.
- Motility:
- Haustral Churning: Local contractions mix contents to facilitate absorption and bacterial fermentation.
- Mass Movements: Powerful, infrequent peristaltic contractions (3-4 times/day, often after meals via gastrocolic reflex) propelling feces toward the rectum.
- Defecation Reflex: Initiated by rectal distension; involves parasympathetic-mediated relaxation of internal anal sphincter and voluntary relaxation of external sphincter and puborectalis muscle.
- Regulation:
- Enteric Nervous System: Controls local motility, secretion, and blood flow via reflexes.
- Autonomic Nervous System:
- Parasympathetic Stimulation: Vagus (proximal colon) and pelvic nerves (distal); enhances motility, secretion, and blood flow.
- Sympathetic Stimulation: Inhibits motility and secretion, constricts sphincters.
- Hormonal Influences: Gastrin, CCK, and motilin stimulate; somatostatin inhibits.
Clinical Considerations
- Understanding abdominal anatomy is critical for diagnosing and managing conditions such as appendicitis (RLQ pain, rebound tenderness), cholecystitis (RUQ pain, Murphy's sign), diverticulitis (LLQ pain, fever), abdominal hernias (e.g., inguinal, umbilical), and bowel obstructions.
- Physical examination techniques, including inspection (for distension, scars), auscultation (bowel sounds), percussion (tympanic vs. dull), and palpation (light/deep for masses, tenderness), rely on knowledge of abdominal organ locations and their functions.
- Imaging studies, such as ultrasound (for gallbladder, kidneys), CT scans (for acute abdomen, tumors), MRI (for soft tissues), and endoscopy, often require an understanding of normal anatomical relationships to identify abnormalities effectively.
- Knowledge of vascular supply is essential in surgical planning (e.g., ligation in colectomy) to prevent inadvertent injury to major blood vessels and ensure adequate perfusion.
- Innervation patterns are important when considering referred pain (e.g., diaphragmatic irritation to shoulder), visceral vs. somatic pain, and the effects of nerve damage or regional anesthesia (e.g., celiac plexus block for pain).
- Nutritional implications: Malabsorption in small intestine diseases (e.g., celiac) vs. electrolyte imbalances in colonic disorders (e.g., diarrhea).
Conclusion
The anatomy of the abdomen is complex, involving multiple organ systems that play essential roles in digestion, absorption, metabolism, immunity, excretion, and homeostasis. A thorough understanding of this anatomy and physiology, including developmental aspects (e.g., midgut rotation), is vital for healthcare professionals in both clinical and surgical settings. It enables accurate diagnosis via history, exam, and imaging; effective treatment planning, including pharmacological, endoscopic, or operative interventions; and the ability to manage complications that may arise during medical interventions, ultimately improving patient outcomes.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery