Lumbar and Sacrum anatomy and function
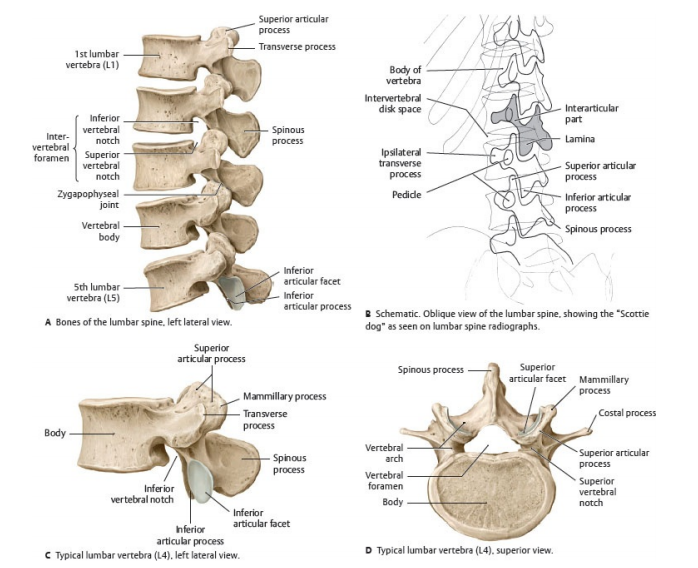
🦴 Lumbar Spine Anatomy
- The lumbar spine consists of five vertebrae (L1–L5), located between the thoracic spine and sacrum.
- Each vertebra has a vertebral body, pedicles, laminae, spinous processes, and transverse processes.
- Intervertebral discs (annulus fibrosus + nucleus pulposus) cushion the vertebrae and act as shock absorbers.
- Facet joints provide stability and controlled movement.
- The spinal canal runs through the vertebrae, protecting the spinal cord and cauda equina.
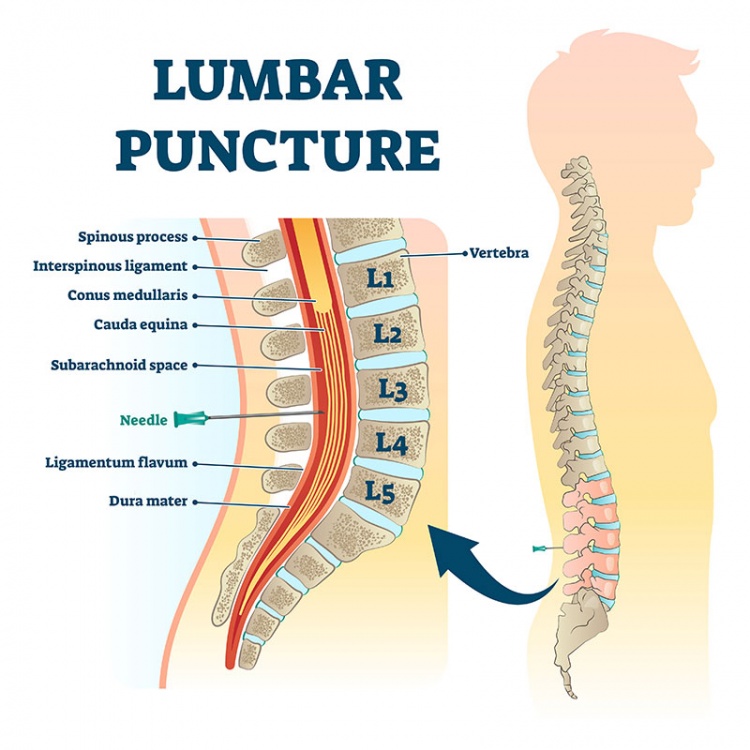
🧠 Contents of the Spinal Canal (Lumbar Level)
- The spinal cord ends at ~L1–L2, forming the conus medullaris.
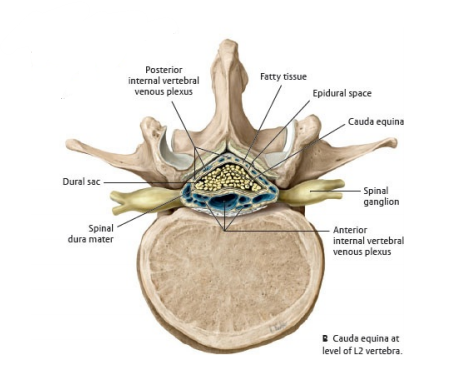
- Below this: the cauda equina (nerve roots supplying legs, bladder, and bowel).
- These roots mediate motor + sensory functions of lower limbs and pelvic organs.
- The dura mater, arachnoid, and pia continue downward as the thecal sac.
- CSF cushions and protects the nerve roots within the lumbar canal.
⚙️ Function of the Lumbar Spine
- Supports the weight of the upper body during sitting/standing.
- Allows movement: flexion, extension, lateral flexion, rotation.
- Provides stability + neural protection.
- Acts as a shock absorber during walking, running, and lifting.
🚨 Common Lumbar Pathologies
- 💥 Herniated Disc: Nucleus pulposus protrudes → nerve compression → sciatica, leg weakness.
- ⏳ Degenerative Disc Disease: Disc wear → stiffness, pain, ↓ flexibility.
- 🔒 Spinal Stenosis: Narrowed canal → leg pain/numbness, worse on walking.
- ↘️ Spondylolisthesis: Vertebral slip forward → back pain, neuro symptoms.
- 🦠 Osteoarthritis: Facet joint degeneration → stiffness, inflammation, chronic pain.
- ⚡ Fractures: Trauma/osteoporosis → instability, severe pain.
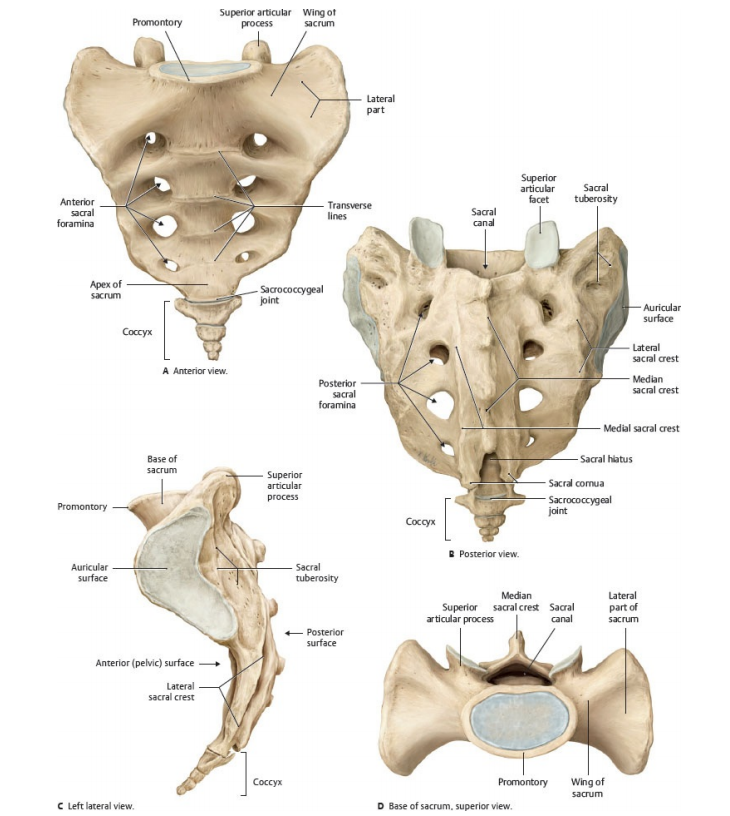
🦴 The sacrum is a large, triangular bone located at the base of the spine, forming the posterior portion of the pelvic girdle.
It sits between the lumbar vertebrae and the coccyx (tailbone).
In humans, the sacrum is composed of five fused vertebrae (S1–S5) that create a single, solid structure, critical for transmitting body weight into the pelvis.
🔎 Key Anatomical Features of the Sacrum
- Base of the Sacrum: The broad upper part, articulating with L5 at the lumbosacral joint.
- Apex of the Sacrum: The narrow lower part connecting with the coccyx.
- Anterior (Pelvic) Surface: Smooth and concave, with four pairs of anterior sacral foramina → passage for anterior sacral nerve branches.
- Posterior Surface: Rough and convex, with the median sacral crest (fused spinous processes), posterior foramina, and tubercles for ligament/muscle attachment.
- Sacral Promontory: The prominent anterior lip of S1 - obstetric landmark for pelvic inlet assessment 👶.
- Auricular Surface: Lateral region articulating with the ilium → forms the strong, weight-bearing sacroiliac joints.
- Sacral Canal: Continuation of the vertebral canal carrying sacral nerve roots (cauda equina). Ends at the sacral hiatus, an important site for caudal epidural anaesthesia 💉.
⚙️ Functions of the Sacrum
- Supports and transmits the weight of the upper body to the pelvis and legs.
- Forms the posterior wall of the pelvic cavity, contributing to pelvic stability.
- Provides foramina for sacral nerves → innervating pelvic organs, perineum, and lower limbs.
- Acts as a keystone in the pelvic arch, stabilising the sacroiliac joints during walking and standing.
🩺 Clinical Relevance
- Sacral Fractures: Usually traumatic (falls, MVAs). May cause nerve compression → urinary/bowel dysfunction or leg weakness.
- Sacroiliac Joint Dysfunction: Painful inflammation or instability of the SI joint → common cause of chronic low back/buttock pain.
- Sacralisation: Congenital fusion of L5 with the sacrum → altered biomechanics, predisposes to back pain.
- Caudal Anaesthesia: Sacral hiatus used for caudal epidural injections in paediatrics & pain management.
- Sacral Tumours: Rare but often present late with pain and neurological deficits due to nerve compression.