
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Sodium Physiology
Related Subjects: |Water Physiology |Sodium Physiology |Potassium Physiology |Aldosterone Physiology |Atrial Natriuretic Peptide (ANP) |Brain Natriuretic Peptide (BNP)
🧂 Sodium (Na⁺) is the dominant extracellular cation and the single most important determinant of extracellular fluid (ECF) volume. A key “exam + clinical” principle is: total body sodium controls volume, while water balance controls sodium concentration. So most hyponatraemia is fundamentally a water excess (ADH problem), whereas most hypernatraemia is a water deficit.
📍 Distribution and why it matters
- Where sodium lives
- ECF (plasma + interstitial fluid): ~135–145 mmol/L (normal lab reference range).
- ICF: ~10–15 mmol/L.
- This steep gradient is essential for membrane potentials, nerve conduction, and coupled transport.
- How the gradient is maintained: Na⁺/K⁺-ATPase
- Pumps 3 Na⁺ out and 2 K⁺ in per ATP → maintains low intracellular Na⁺ and contributes to a negative resting membrane potential.
- Creates the “stored energy” used by secondary active transport (e.g. glucose uptake in the gut, renal reabsorption).
🧠 Sodium, osmolality, and brain adaptation (high-yield)
- Tonicity vs osmolality
- Osmolality = total dissolved particles per kg water (includes urea).
- Tonicity (effective osmolality) = particles that do not freely cross cell membranes and therefore shift water (mainly Na⁺ and glucose).
- That’s why hyperglycaemia can cause “dilutional” hyponatraemia (water shifts out of cells).
- Why rapid Na correction is dangerous
- In chronic hyponatraemia, brain cells adapt by expelling osmoles to reduce cerebral oedema.
- If you raise serum Na⁺ too fast, water rapidly leaves brain cells → risk of osmotic demyelination syndrome (ODS).
- In acute hyponatraemia, there’s less time to adapt → cerebral oedema and seizures are the main threat.
⚙️ Key physiological functions of sodium
- ECF volume and blood pressure
- Sodium content of ECF drives water retention → determines circulating volume and therefore perfusion pressure.
- Chronic sodium excess contributes to hypertension via volume expansion and vascular remodelling.
- Electrical excitability (nerve and muscle)
- Fast Na⁺ influx through voltage-gated channels generates the upstroke of action potentials in neurons and skeletal muscle.
- In cardiac tissue, Na⁺ is crucial for phase 0 depolarisation (esp. atrial/ventricular myocytes and Purkinje fibres).
- Secondary active transport
- Gut: SGLT1 co-transports Na⁺ + glucose (basis of oral rehydration therapy).
- Kidney: Na⁺ gradients power multiple solute transporters along the nephron.
- Acid–base physiology (advanced but useful)
- Na⁺ is the major “strong cation”; changes in accompanying anions (especially chloride) influence acid–base balance.
- Large volumes of 0.9% saline (high chloride) can contribute to hyperchloraemic metabolic acidosis, hence interest in balanced crystalloids in some settings.
🧪 Renal handling of sodium (where it’s reabsorbed + key transporters)
- Filtered load
- Na⁺ is freely filtered at the glomerulus; the kidney then “chooses” how much to reclaim.
- Small changes in fractional excretion make big differences in volume status.
- Proximal tubule (~65% reabsorbed)
- Major transporter: NHE3 (Na⁺/H⁺ exchanger) + Na⁺ co-transport with glucose, amino acids, phosphate.
- “Iso-osmotic reabsorption”: water follows solute → preserves tonicity.
- Thick ascending limb (~25%)
- Major transporter: NKCC2 (Na⁺-K⁺-2Cl⁻ cotransporter).
- Water-impermeable → helps create the medullary gradient (countercurrent multiplication).
- Loop diuretics act here.
- Distal convoluted tubule (~5%)
- Major transporter: NCC (Na⁺-Cl⁻ cotransporter).
- Thiazides act here and are a classic cause of hyponatraemia.
- Collecting duct (~2–3% but “fine-tuning”)
- Major channel: ENaC (epithelial Na⁺ channel), stimulated by aldosterone.
- Coupled to K⁺ and H⁺ secretion → explains hyperkalaemia and acidosis risk in hypoaldosteronism.
- Amiloride blocks ENaC; spironolactone/eplerenone block mineralocorticoid receptor.
🧠 Hormonal control: sodium balance vs sodium concentration
- RAAS (renin–angiotensin–aldosterone system)
- Triggered by low effective arterial blood volume (EABV): renal hypoperfusion, low NaCl delivery to macula densa, sympathetic activation.
- Angiotensin II: vasoconstriction + increases proximal Na⁺ reabsorption + stimulates aldosterone and thirst.
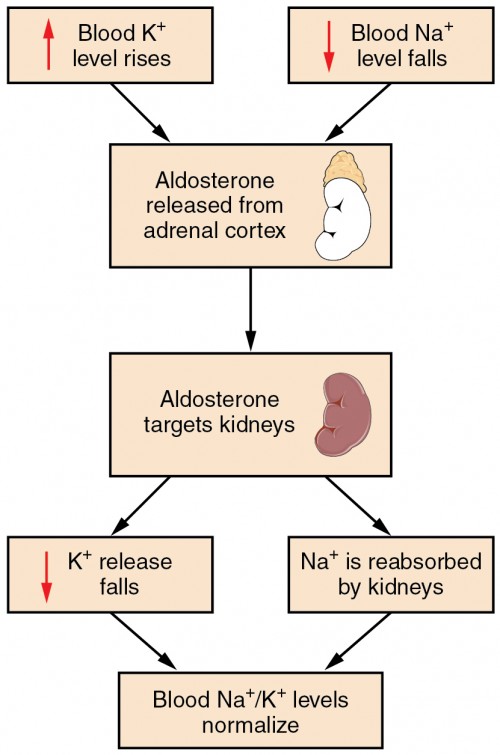
- Aldosterone: increases ENaC and Na⁺/K⁺-ATPase activity → Na⁺ retention (with K⁺/H⁺ loss).
- Natriuretic peptides (ANP/BNP)
- Released with atrial/ventricular stretch → promote natriuresis and vasodilation, suppress renin/aldosterone.
- ADH (vasopressin): mainly water, not sodium
- Increases water reabsorption in collecting duct via aquaporin-2 insertion.
- Therefore ADH changes serum Na⁺ concentration by changing water balance.
- Thirst
- Osmoreceptors in hypothalamus respond to small rises in tonicity → drives water intake.
- In frail older adults, impaired thirst/access to water is a common hypernatraemia mechanism.
🏥 Clinical approach to abnormal sodium (the framework that wins exams)
1) Hyponatraemia (Na⁺ <135)
- Step 1: check osmolality
- Hypotonic hyponatraemia (most common): true water excess.
- Isotonic: pseudohyponatraemia (very high lipids/protein; lab artifact with some methods).
- Hypertonic: translocational hyponatraemia (e.g., hyperglycaemia, mannitol).
- Step 2: assess volume status clinically
- Hypovolaemic: GI losses, diuretics, adrenal insufficiency, renal salt wasting.
- Euvolaemic: SIADH, hypothyroidism, glucocorticoid deficiency, primary polydipsia.
- Hypervolaemic: heart failure, cirrhosis, nephrotic syndrome (low EABV → high ADH despite oedema).
- Step 3: use urine studies to “read ADH and aldosterone”
- Urine osmolality:
- <100 mOsm/kg suggests suppressed ADH (e.g., primary polydipsia, low solute intake).
- >100 mOsm/kg suggests ADH is active (common in SIADH, hypovolaemia, heart failure).
- Urine sodium (often with a threshold around 30 mmol/L):
- Low urine Na⁺ suggests kidneys avidly retaining sodium (low EABV states).
- Higher urine Na⁺ suggests renal sodium loss or SIADH pattern.
- Urine osmolality:
- Symptoms (brain swelling = the danger)
- Mild: nausea, headache, gait instability.
- Severe: confusion, seizures, coma (treat as emergency).
Emergency hyponatraemia (what you actually do)
- If seizures or severe neurological symptoms: give hypertonic saline in controlled boluses with frequent Na⁺ checks.
- Targets are modest early rises (e.g., ~4–6 mmol/L) to relieve cerebral oedema, then slow correction to avoid ODS.
- Do not “normalise” sodium quickly - you are treating brain oedema first, not the lab number.
2) Hypernatraemia (Na⁺ >145)
- Core concept: almost always water deficit relative to sodium.
- Common causes
- Reduced intake: impaired thirst, reduced access to water, delirium.
- Excess losses: diarrhoea, sweating, burns, osmotic diuresis (e.g., hyperglycaemia).
- Diabetes insipidus: inadequate ADH (central) or renal resistance (nephrogenic).
- Treatment principle
- If shocked/hypovolaemic: resuscitate first (isotonic fluid), then replace free water.
- Correct gradually if chronicity uncertain to reduce cerebral oedema risk.
💉 Sodium content of common IV fluids (practical prescribing)
- 0.9% sodium chloride: ~154 mmol/L sodium (and 154 mmol/L chloride).
- 3% sodium chloride: very concentrated hypertonic saline (~513 mmol/L sodium).
- In hyponatraemia, giving isotonic saline may raise Na⁺ very little directly, but can stop hypovolaemia-driven ADH → brisk water diuresis and a faster-than-expected Na rise (watch for overcorrection).
📝 Summary
Sodium is the main extracellular cation and the key determinant of extracellular volume and perfusion. The kidneys fine-tune sodium via segment-specific transporters (PT → TAL → DCT → collecting duct) under RAAS and natriuretic peptide control, while ADH and thirst primarily regulate water and therefore sodium concentration. Clinically, think in frameworks: hyponatraemia = check tonicity → assess volume → urine osm/Na; hypernatraemia = water deficit. In emergencies, treat the brain first (seizures/cerebral oedema) and correct sodium slowly enough to avoid iatrogenic neurological injury.
🔗 Useful UK-friendly links: | NICE CKS: Hyponatraemia | NICE CG174: IV fluids in adults | Society for Endocrinology (2022): emergency hyponatraemia
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery