
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Vascular Surgery: Introduction
Related Subjects: | Vascular Surgery: Introduction | Ankle-Brachial Pressure Index (ABPI) and Peripheral Vascular Disease | Peripheral Arterial Disease (PAD) | Abdominal Aortic Aneurysm (AAA) | Carotid Endarterectomy | Buerger's disease (Thromboangiitis obliterans) | Leriche syndrome (aortoiliac occlusive disease)
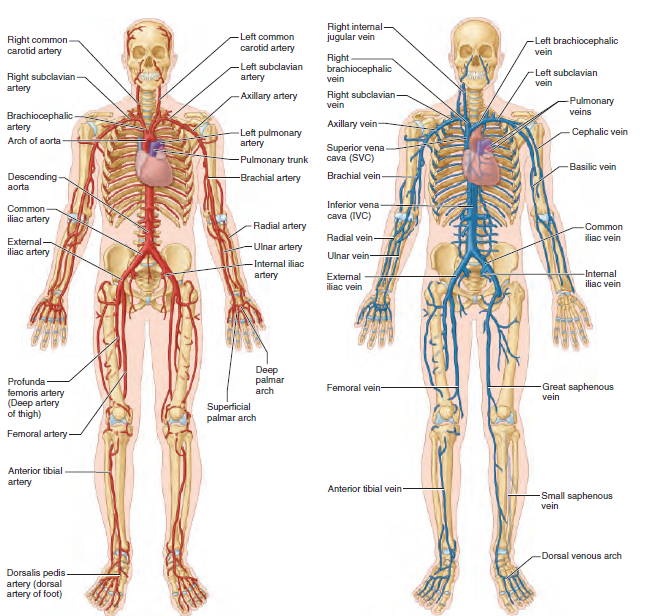
🧠 Anatomy
🩺 Vascular Surgery - Introduction (Principles)
🩸 Vascular surgery is the surgical and endovascular management of diseases of the arteries, veins, and lymphatics (most commonly driven by atherosclerosis, thrombosis/embolism, aneurysm disease, and venous reflux). 🎯 The core aim is simple: maintain or restore perfusion, prevent stroke, prevent limb loss, and reduce cardiovascular death by combining procedures with aggressive risk-factor control.
- 🧭 “Treat the patient, not just the vessel”: PAD and aneurysm disease are markers of systemic atherosclerosis → every vascular patient needs secondary prevention (smoking cessation 🚭, statin 💊, antiplatelet 🩹 where appropriate, BP/diabetes control).
- ⚖️ Balance risk vs benefit: interventions are chosen when the benefit (symptom relief, limb salvage, rupture prevention) outweighs peri-operative risk (cardiac, renal, bleeding, infection).
- 🧰 Two toolkits: endovascular (angioplasty/stent, thrombolysis, EVAR) and open surgery (bypass, endarterectomy, open aneurysm repair).
- 🔁 Good vascular practice is iterative: assess → stabilise → image → intervene → reassess (perfusion, pain, wounds, function), with early escalation when deterioration occurs.
🚨 Time-Critical Vascular Problems (recognise early)
| Condition | Why it matters | First priorities (exam/ward-ready) |
|---|---|---|
| ⚡ Acute limb ischaemia | Sudden loss of arterial supply → limb loss risk within hours | ABC + analgesia, keep limb dependent, urgent senior/vascular referral, anticoagulate if appropriate per protocol, rapid imaging/planning |
| 🧨 Ruptured / symptomatic AAA | High mortality; time-critical haemorrhage control | Resus, permissive hypotension approach per local policy, activate major haemorrhage, urgent CTA if stable enough |
| 🦶 Critical limb-threatening ischaemia (CLTI) | Rest pain/tissue loss + poor perfusion → infection/amputation risk | Analgesia, sepsis screen if infected ulcer, protect wounds, urgent vascular assessment for revascularisation planning |
| 🧠 Carotid disease with symptoms | Stroke risk is front-loaded after TIA/stroke | Urgent stroke/TIA pathway + carotid imaging; specialist decision re endarterectomy/stenting |
🧪 Vascular Investigations (what they tell you)
🦶 Ankle–Brachial Pressure Index (ABPI)
The ABPI is the ratio of ankle systolic pressure to brachial systolic pressure, used to estimate peripheral arterial perfusion. It is most helpful when interpreted alongside symptoms (claudication vs rest pain), pulse findings, and tissue loss - the clinical picture matters more than a single number.
🧠 Technique pearl: measure brachial systolic (both arms; use the higher), then ankle systolic at dorsalis pedis and posterior tibial with Doppler; use the higher ankle value for each leg. ⚠️ ABPI can be falsely high in calcified, incompressible arteries (e.g., diabetes, CKD, vasculitis) - in that setting consider toe pressures/toe-brachial index or vascular lab assessment.
📊 ABPI interpretation
| Resting ABPI | Likely interpretation | Clinical correlation |
|---|---|---|
| > 1.3 | Suggests arterial calcification / incompressible vessels | Common in diabetes, CKD, RA/vasculitis → ABPI may be unreliable |
| 0.8 – 1.3 | No evidence of significant PAD | Compression stockings generally safe (if no other contraindications) |
| 0.5 – 0.8 | Moderate PAD | Often intermittent claudication; optimise risk factors + consider imaging if severe symptoms |
| < 0.5 | Severe ischaemia | Often critical ischaemia/rest pain or tissue loss → urgent vascular input |
🟦 Duplex ultrasonography
A non-invasive test combining grey-scale ultrasound (structure) with Doppler (flow) to characterise direction, velocity, and turbulence. It is a workhorse investigation for PAD (stenosis/occlusion mapping), venous insufficiency (reflux), and DVT.
- ✅ Pros: bedside-friendly, no radiation, no contrast.
- ⚠️ Limits: operator-dependent; can be harder in obesity, bowel gas, heavy calcification.
🖥️ CT angiography (CTA)
CTA visualises arterial and venous anatomy using IV contrast and allows 3D reconstruction for operative planning (stenosis, aneurysm, dissection, trauma). It is fast and widely available, which is why it’s heavily used in emergencies and pre-procedure mapping.
- ⚠️ Cons: ionising radiation; contrast nephrotoxicity risk and allergy considerations.
- 💡 OSCE line: “Check eGFR, allergy history, and metformin/contrast policy as per local guidance.”
🦶 Ulcers arterial vs venous vs neuropathic vs pressure
🧠 A leg/foot ulcer is a diagnostic problem first, then a dressing problem. Always document: site, size, depth, exudate, odour, surrounding skin, pulses, capillary refill, neuropathy, and infection signs.
- Differentials to remember: skin cancer, pyoderma gangrenosum, necrobiosis lipoidica, vasculitis.
| Ulcer type | Typical clues | Management principles |
|---|---|---|
| 🟥 Arterial | Painful, punched-out, distal (toes/foot), cool limb, reduced pulses, low ABPI | 🚭 Smoking cessation is paramount; optimise risk factors (statin + antiplatelet if appropriate). 🧭 Plan imaging for revascularisation (endovascular/open) ± debridement once perfusion improved. ⛔ Compression is contraindicated. |
| 🟫 Venous | Medial gaiter area, shallow, exudative, oedema, eczema/haemosiderin, pulses present | 🧦 Compression therapy + elevation; consider pentoxifylline as adjunct in some cases. 🩺 Treat underlying venous pathology (e.g., varicose vein intervention) and optimise skin care. |
| 🟨 Neuropathic (diabetic) | Plantar pressure points, callus, reduced sensation, warm foot, may have pulses | 👣 Podiatry for offloading (casts/footwear), debridement and regular dressings. 🦠 Treat infection early; assess perfusion too (neuro-ischaemic ulcers are common). |
| 🟦 Pressure | Over bony prominences, immobility, tissue injury signs | 🛏️ Nursing/tissue viability involvement; frequent repositioning, pressure-relieving surfaces, dressings, debridement when appropriate. 🍽️ Optimise nutrition and moisture control; consider negative-pressure therapy in selected wounds. |
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery