Abdominal paracentesis for ascites
Abdominal paracentesis is a bedside procedure to remove ascitic fluid, either for diagnosis (e.g. rule out spontaneous bacterial peritonitis, SBP) or therapy (to relieve tense ascites).
💡 Always consider diagnostic paracentesis on admission in a cirrhotic patient with ascites - SBP can be silent but life-threatening.
🧠 Pathophysiology Context
- Ascites is most commonly due to portal hypertension from cirrhosis → raised hydrostatic pressure + low oncotic pressure (hypoalbuminaemia) → fluid transudation.
- Other causes: malignancy, TB peritonitis, cardiac failure, pancreatitis.
- Paracentesis relieves intra-abdominal pressure, improving breathing, appetite, and comfort.
📌 About
- Diagnostic paracentesis: Small volume for fluid analysis (protein, SAAG, culture).
- Therapeutic paracentesis: Large-volume drainage (>5 L) for symptom relief.
- Routine coagulation or platelet testing is not required unless high bleeding risk (per guidelines).
✅ Indications
- All cirrhotic patients with ascites on admission (rule out SBP).
- New-onset ascites of uncertain cause.
- Clinical deterioration: fever, abdominal pain, encephalopathy, renal failure.
- Symptomatic tense ascites requiring relief.
🚫 Contraindications
- Severe uncorrectable coagulopathy (INR >1.5, platelets <40 ×109/L).
- Distended bowel from obstruction, infected abdominal wall at puncture site.
- Relative: pregnancy, abdominal wall collaterals, large intra-abdominal masses.
⚠️ Cautions
- Hyponatraemia, renal impairment, anaemia, hypoalbuminaemia (<20 g/L).
- Poor cooperation, prior surgery with adhesions, pregnancy (USS guidance essential).
🔎 Complications
- Bleeding - intra-abdominal haemorrhage can be fatal.
- Bowel perforation → peritonitis.
- Persistent fluid leak from puncture site.
- Post-paracentesis circulatory dysfunction → hypotension, hyponatraemia.
🛠️ Procedure Essentials
- Consent, identity check, baseline obs, IV access.
- Empty bladder (void/catheterise).
- Position: supine, head on pillow.
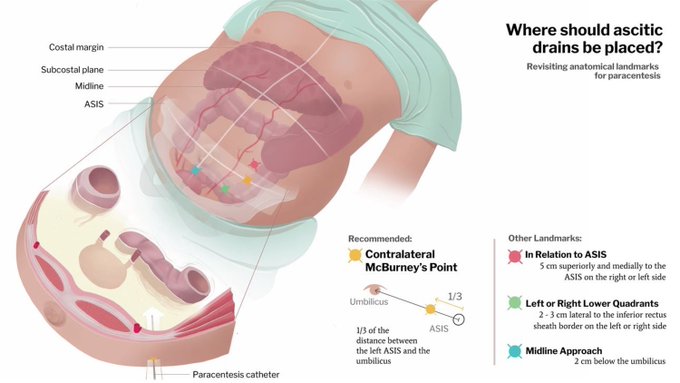
- Site: left lower quadrant, lateral to rectus sheath; USS guidance reduces risk.
- Clean skin, drape sterile field. Anaesthetise skin & peritoneum (lidocaine).
- Use Z-track technique to reduce post-drain leakage.
🔬 Investigations from Ascitic Fluid
- SAAG (Serum-Ascites Albumin Gradient):
- ≥1.1 g/dL → portal hypertension (cirrhosis, heart failure).
- <1.1 g/dL → malignancy, TB, pancreatitis.
- Culture & microscopy (ascitic neutrophils >250/mm³ = SBP).
- Total protein (low in cirrhosis; high in malignancy, TB).
- Additional: cytology, amylase, BNP, ADA depending on suspicion.
💉 Post-Procedure Care
- Albumin infusion: Give 8 g per litre drained if >5 L removed (e.g. 20% albumin) to prevent circulatory dysfunction.
- For SBP with renal risk: 1.5 g/kg albumin on day 1, then 1 g/kg on day 3.
- Monitor vitals, puncture site, urine output.
⏱️ Drain Duration
- Usually removed after fluid evacuation (same day, within a few hours).
- Large-volume (>8 L): may need staged removal.
- Not usually left >24 h - infection and leakage risk rises significantly.
💡 Clinical Pearl: Do not delay diagnostic paracentesis in cirrhotic patients with ascites + fever or encephalopathy while awaiting clotting results. Early diagnosis and treatment of SBP improves survival.
📚 References
