
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Prostate cancer✅
Related Subjects: | Urothelial Tumours | Haematuria | Acute Urinary Retention | Anuria and Oliguria | Bladder Cancer |Penile Cancer | Renal Cell Carcinoma | Benign Prostatic Hyperplasia | IgA Nephropathy | Prostate Cancer | Henoch-Schonlein Purpura | Glomerulonephritis
🧪 PSA (Prostate-Specific Antigen) is a protein produced by epithelial cells of the prostate gland. ⚗️ It is a 34 kDa serine protease glycoprotein that helps liquefy semen.
- 📈 PSA can rise in prostate cancer, benign prostatic hyperplasia (BPH), prostatitis, urinary retention, and increasing age.
- ⏱️ PSA velocity refers to the rate of PSA change over time and may suggest malignancy if rapidly rising.
- 🦴 Very high PSA levels (often >100 ng/mL) strongly suggest metastatic disease, particularly bone metastases.
- ✋ Digital rectal examination (DRE) does not significantly elevate PSA.
- ⚠️ PSA is not cancer-specific; interpretation requires clinical context.
📌 About Prostate Cancer
- 🧓 Most common cancer in men in the UK.
- 📈 Incidence increases sharply with age.
- 🔍 Many tumours are slow growing and may never cause symptoms.
- ⚖️ The clinical challenge is balancing early detection with avoiding overtreatment.
- 💉 Tumour growth is typically androgen-dependent (driven by testosterone).
📊 Epidemiology
- 🇬🇧 Around 52,000 new cases per year in the UK.
- 👨 Rare before age 50.
- 🏿 Risk is significantly higher in Black African and Caribbean men.
- 👨👦 Family history increases risk (≈2–3×).
- ⚖️ Obesity and smoking are associated with more aggressive disease.
🧫 Pathology
- 🧬 ~95% are acinar adenocarcinomas arising from glandular epithelium.
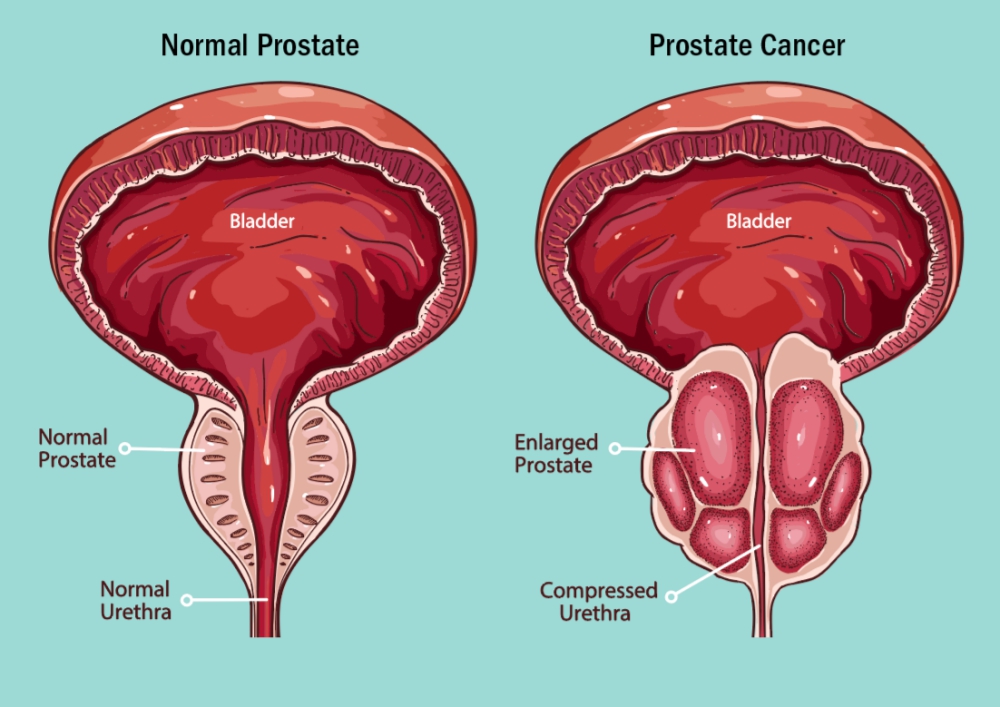
- 📍 Most tumours arise in the peripheral zone of the prostate.
- 🧪 Prostatic intraepithelial neoplasia (PIN) is a recognised precursor lesion.
- 🧬 Tumour aggressiveness is graded using the Gleason scoring system.
🩺 Clinical Presentation
- 💧 Lower urinary tract symptoms (LUTS) frequency, nocturia, weak stream, hesitancy
- 🩸 Haematuria or haematospermia
- 🦴 Bone pain → may indicate metastatic disease
- ⚠️ Many patients are asymptomatic at diagnosis
🧩 Common Clinical Findings
- 📈 Raised PSA on blood testing
- ✋ DRE findings: hard, irregular or nodular prostate
- 🚽 Bladder outflow obstruction → possible renal impairment
- 🦴 Osteosclerotic bone metastases causing pain or pathological fracture
📐 PSA Reference Ranges (Age-Adjusted)
- 👨 40–49 yrs: <2.5 ng/mL
- 👨 50–59 yrs: <3.5 ng/mL
- 👨 60–69 yrs: <4.5 ng/mL
- 👨 ≥70 yrs: <6.5 ng/mL
- 📊 PSA 4–10 ng/mL → cancer risk ≈25%
- 📊 PSA >10 ng/mL → higher risk of malignancy
- 🎗️ Prostate cancer
- 🟢 Benign prostatic enlargement / BPH
- 🔥 Prostatitis
- 🦠 Urinary tract infection
- 🚫 Acute urinary retention
- 🧪 Recent catheterisation, cystoscopy, prostate biopsy or instrumentation
- 🚴 Recent ejaculation, cycling or vigorous exercise
- 👴 Increasing age and larger prostate volume
🔍 Investigations
- 🩸 Blood tests: U&E, FBC, ALP (may rise with bone metastases)
- 📡 Multiparametric MRI (mpMRI) is now performed before biopsy in suspected prostate cancer.
- 🧪 Targeted prostate biopsy (usually transperineal) guided by MRI findings.
- 📊 Gleason score / Grade Group used to determine tumour aggressiveness.
- 🦴 Bone scan or PSMA-PET if high PSA, high Gleason score, or symptoms suggesting metastases.
📊 Risk Stratification (Localised Disease)
| Risk Level | PSA | Gleason Score | Clinical Stage |
|---|---|---|---|
| Low | <10 | ≤6 | T1–T2a |
| Intermediate | 10–20 | 7 | T2b |
| High | >20 | 8–10 | ≥T2c |
🛠️ Management (UK Practice – NICE NG131)
📌 Initial Assessment
- Risk stratification using PSA, MRI findings, Gleason score, and stage.
- All cases discussed at specialist multidisciplinary team (MDT).
🏥 Localised Disease (T1–T2)
Low-risk disease- 👀 Active surveillance is often preferred.
- Definitive treatment if progression occurs.
- 🔪 Radical prostatectomy
- 🎯 External beam radiotherapy ± short-course androgen deprivation therapy
- ⚡ Brachytherapy in selected patients
- 🎯 Radiotherapy + long-term androgen deprivation therapy (ADT)
- 🔪 Surgery considered in selected patients in specialist centres
📍 Locally Advanced Disease (T3–T4)
- 🎯 External beam radiotherapy + long-term ADT
- Multimodal treatment often required
🌍 Metastatic Disease
Hormone-sensitive metastatic disease- 💉 Androgen deprivation therapy (ADT) (LHRH agonist or antagonist)
- ➕ Treatment intensification with docetaxel, abiraterone, enzalutamide, or apalutamide
- Continue ADT
- ➕ novel hormonal therapies or chemotherapy
- 🦴 Radium-223 for symptomatic bone metastases
- 🧬 PARP inhibitors (e.g. olaparib) for BRCA-mutated cancers
🤝 Supportive Care
- 🦴 Bone protection: bisphosphonates or denosumab
- 💪 Manage ADT complications (osteoporosis, metabolic syndrome, fatigue)
- 🎯 Palliative radiotherapy for painful bone metastases
🇬🇧 UK Practice Points
- Follow NICE NG131 guidance.
- mpMRI is recommended before biopsy.
- All treatment decisions made via MDT discussion.
- 📊 Long-term PSA monitoring after treatment is essential.
🩺 Case 1 – Low-risk Prostate Cancer
A 62-year-old man has PSA 6.1 ng/mL detected in primary care. MRI shows a small PIRADS-3 lesion and biopsy confirms Gleason 3+3 disease. Management: Active surveillance with regular PSA monitoring, MRI follow-up, and repeat biopsy if disease progression is suspected.
🩺 Case 2 – Intermediate-risk Disease
A 68-year-old man presents with PSA 12.8 ng/mL and MRI showing a PIRADS-5 lesion. Biopsy confirms Gleason 4+3 cancer. Management: Radical prostatectomy or external beam radiotherapy with short-term androgen deprivation therapy.
🩺 Case 3 – Metastatic Prostate Cancer
A 74-year-old man presents with back pain and PSA 186 ng/mL. Imaging confirms multiple bone metastases. Management: Androgen deprivation therapy combined with systemic therapy (e.g. abiraterone or docetaxel), with palliative radiotherapy for symptomatic bone metastases.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery