Related Subjects:
|High Altitude Physiology
|Diving Physiology
|Trauma Physiology
|Exercise Physiology
|Gastric Physiology
|Rectal Physiology
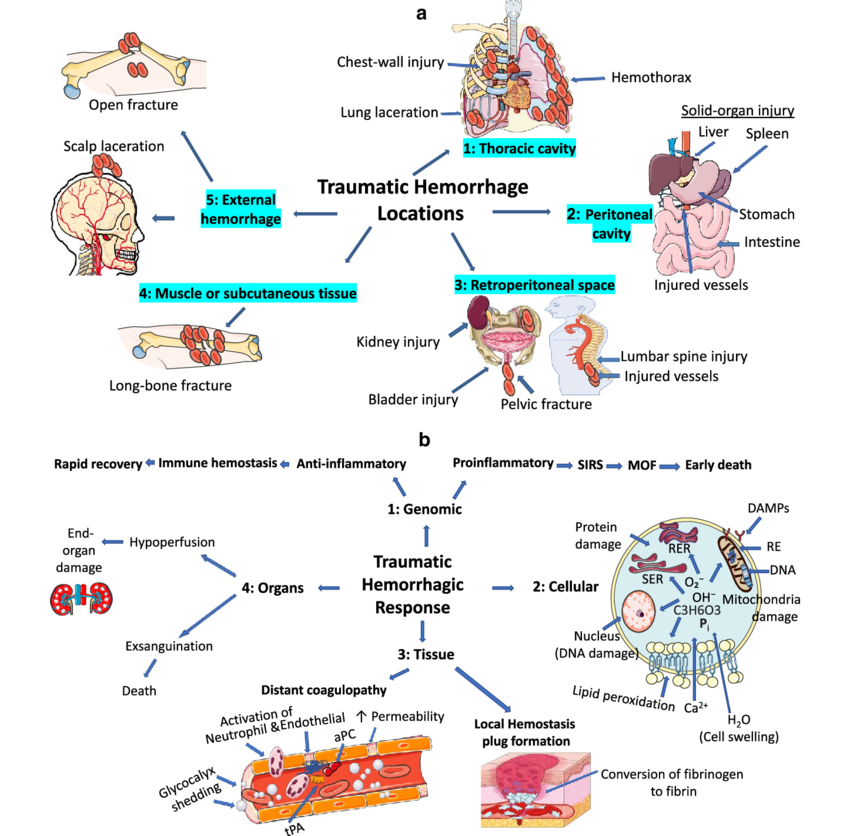
🩸 Trauma physiology examines how the body responds to severe injury.
Understanding these responses is crucial for effective trauma care: stabilising vital functions, preventing secondary injury, and optimising recovery.
⚡ Physiological Responses to Trauma
- Haemodynamic Changes:
- 🩸 Hypovolemic Shock: Severe blood loss ↓ circulating volume → inadequate perfusion and oxygen delivery.
- 🫀 Vasoconstriction: Peripheral vasoconstriction maintains cerebral and coronary perfusion.
- 💓 Tachycardia: Compensatory mechanism to sustain cardiac output, though may fail with prolonged bleeding.
- Inflammatory Response:
- 🔥 Cytokine Release: TNF-α, IL-1, and IL-6 drive systemic inflammatory response (SIRS).
- 🦠 Leukocyte Activation: Migration to injured tissues for repair and infection control.
- 🧬 Coagulation Cascade: Activation of clotting pathways; risk of trauma-induced coagulopathy if dysregulated.
- Metabolic Response:
- ⚡ Hypermetabolism: Catecholamine surge ↑ resting energy expenditure.
- 🍖 Catabolism: Muscle and fat breakdown → energy substrate but worsens muscle wasting.
- 🩺 Insulin Resistance: Stress response causes hyperglycaemia, which can impair wound healing.
🕑 Phases of Trauma Response
- Immediate Phase (Minutes–Hours):
- 🩹 Control bleeding, maintain perfusion (Airway, Breathing, Circulation).
- Shock response: catecholamines and vasoconstriction dominate.
- Acute Phase (Hours–Days):
- Ongoing resuscitation, stabilisation, and correction of metabolic derangements.
- Systemic inflammatory response peaks, risk of sepsis and coagulopathy.
- Chronic Phase (Days–Weeks):
- Focus shifts to wound healing, rehabilitation, and psychological recovery.
- Risk of malnutrition, sarcopenia, PTSD.
🫁 Key Organ Systems Affected
- Cardiovascular: Maintain perfusion, prevent exsanguination. Uncorrected shock → MODS.
- Respiratory: Risk of pneumothorax, pulmonary contusion, ARDS. Prioritise oxygenation.
- Renal: Trauma + hypoperfusion → prerenal AKI. Beware rhabdomyolysis releasing myoglobin.
- Nervous: Traumatic brain injury (TBI), spinal cord injury. Raised ICP → secondary brain injury if untreated.
🛠️ Trauma Assessment & Management
- Primary Survey (ABCDE):
- 🅰️ Airway: With c-spine protection.
- 🅱️ Breathing: Ventilation, chest drains for pneumothorax/haemothorax.
- 🅲️ Circulation: Control haemorrhage, restore volume (balanced resuscitation with blood products).
- 🅳️ Disability: Neuro assessment (AVPU, GCS).
- 🅴️ Exposure: Full exposure to find injuries, prevent hypothermia.
- Secondary Survey: Head-to-toe exam, imaging, history (AMPLE: Allergies, Meds, Past history, Last meal, Events).
- Resuscitation: Blood transfusion, TXA (within 3 hours), vasopressors if refractory shock.
⚠️ Complications
- ARDS: Inflammatory lung damage → impaired oxygenation.
- Sepsis & MODS: Secondary infections worsen outcomes.
- Trauma-Induced Coagulopathy: “Lethal triad” of hypothermia, acidosis, coagulopathy.
- Compartment Syndrome: 🚨 Orthopaedic emergency → requires fasciotomy.
💪 Recovery & Rehabilitation
- 🏃 Physiotherapy: Regain strength and mobility.
- 🧠 Psychological Support: PTSD, anxiety, and depression common after major trauma.
- 🧑🦽 Occupational Therapy: Assist return to independence and work.
- 📅 Follow-up: Ongoing monitoring for renal, neuro, and cardiac sequelae.
📌 Summary
Trauma physiology integrates shock, inflammation, and metabolic stress.
Effective care requires rapid resuscitation, vigilant monitoring of organ systems, and multidisciplinary rehabilitation.
A trauma team must anticipate complications early - survival depends on recognising patterns of physiology as much as on treating the injuries themselves.
