
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Osteogenic sarcoma (Osteosarcoma)
Related Subjects: |Osteogenic sarcoma (Osteosarcoma) |Ewing sarcoma
🦴⚡ Osteosarcoma is the most common primary malignant bone tumour of adolescence. It is radio-resistant ❌, so radiotherapy is usually not part of the treatment plan.
📖 About
- Most common primary malignant bone tumour in adolescents & young adults (peak age 15–18).
- Arises in the metaphysis of long bones near growth plates (rapid growth zones during puberty).
- Produces immature bone (osteoid) as its pathological hallmark.
- Most common sites: distal femur, proximal tibia, proximal humerus.
🧬 Aetiology & Genetics
- Genetic predisposition:
- Li-Fraumeni syndrome (TP53 mutation) 🧬
- Hereditary retinoblastoma (RB1 gene) 👁️
- Other associations:
- Paget’s disease of bone (older adults) 🦴
- Prior exposure to ionising radiation ☢️
- Pathology: malignant cells producing disorganised osteoid → bone destruction & replacement.
🩺 Clinical Features
- Persistent, progressive pain (often worse at night) 😣.
- Swelling & tenderness around the joint.
- Palpable, firm mass in advanced cases.
- Restricted joint movement; limp if lower limb affected.
- Pathological fracture due to weakened bone 🦴💥.
- Systemic symptoms (weight loss, fever, malaise) usually appear late.
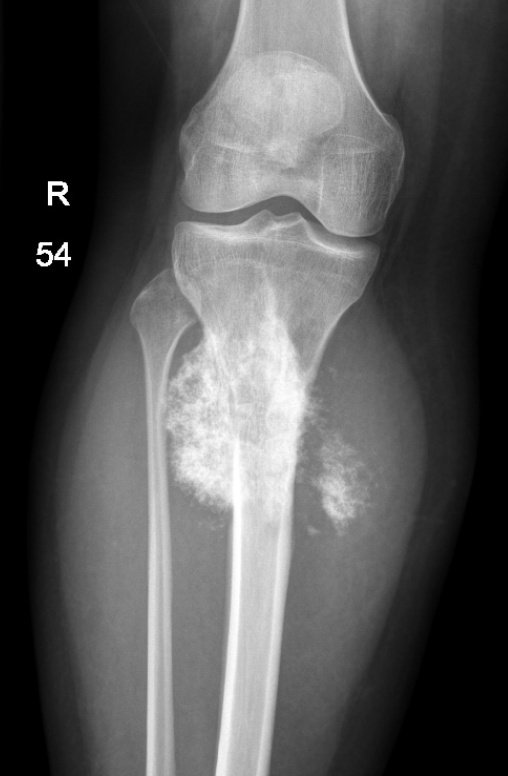
🖼️ Classic Imaging Signs
- Plain X-ray: “Sunburst appearance” 🌞 = spiculated periosteal bone growth.
- Codman’s Triangle: periosteal elevation due to aggressive tumour growth 📐.
- MRI: Defines local extent & soft-tissue invasion (surgical planning).
- CT chest: Essential to look for lung metastases (most common site 🌬️).
🧪 Other Investigations
- Biopsy: Core/open biopsy = gold standard for histological diagnosis.
- Labs: ↑ Alkaline phosphatase & LDH → correlate with tumour burden & prognosis.
- Bone scan: Detects multifocal disease or bone metastases.
💊 Treatment
- Surgery: Mainstay of treatment 🩺✂️
- Limb-salvage surgery now preferred in many cases.
- Amputation still used if tumour encases vital neurovascular structures.
- Chemotherapy: 💉
- Given pre-operatively (neoadjuvant) to shrink tumour.
- Post-operatively (adjuvant) to eliminate micrometastases.
- Common agents: Methotrexate, Doxorubicin, Cisplatin, Ifosfamide (MAP regimen).
- Radiotherapy: ❌ Not effective (radio-resistant).
📈 Prognosis
- With modern therapy: 5-year survival for localised disease ≈ 60–70% 🌟.
- Poorer outcomes in:
- Axial tumours (pelvis/spine/skull).
- Metastatic disease at diagnosis (esp. lungs) 🌬️.
- Poor histological response to neoadjuvant chemo.
🧑🏫 Exam Tip
Remember the triad for imaging OSCEs: Sunburst pattern 🌞, Codman’s triangle 📐, and metaphyseal location near growth plates. Always link osteosarcoma to adolescents with bone pain + swelling and highlight that radiotherapy is not used 🚫.
📚 References
- Oxford Handbook of Oncology
- Campbell’s Operative Orthopaedics
Cases - Osteogenic Sarcoma (Osteosarcoma)
- Case 1 - Adolescent with knee pain 🦴: A 15-year-old boy presents with progressive pain and swelling around his left knee, worse at night and not relieved by rest. Exam: firm, tender mass around distal femur. X-ray: mixed lytic–sclerotic lesion with periosteal elevation (“sunburst” pattern, Codman’s triangle). Diagnosis: osteosarcoma of distal femur. Managed with neoadjuvant chemotherapy followed by limb-salvage surgery.
- Case 2 - Pathological fracture ⚡: A 17-year-old girl presents after a minor fall causing a mid-femoral fracture. History: 3 months of dull bone pain. X-ray: destructive metaphyseal lesion with cortical breach. Biopsy: malignant osteoid production. Diagnosis: osteosarcoma presenting with pathological fracture. Managed with chemo and surgical resection; orthopaedic oncology team involved.
- Case 3 - Metastatic disease 🌬️: A 14-year-old boy with known osteosarcoma of the proximal tibia (diagnosed 6 months ago) presents with cough and breathlessness. CT chest: multiple cannonball pulmonary metastases. Diagnosis: osteosarcoma with lung metastases. Managed with systemic chemotherapy, resection of primary tumour, and palliative resection of lung mets if feasible.
Teaching Point 🩺: Osteosarcoma is the most common primary malignant bone tumour in adolescents, usually affecting metaphyses of long bones (distal femur, proximal tibia, proximal humerus). Key features: progressive bone pain, swelling, pathological fractures. X-ray: sunburst periosteal reaction, Codman’s triangle. Metastasis: commonly to lungs. Management: multi-agent chemotherapy + surgical resection (limb-salvage or amputation).



| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery