Related Subjects:
|Olfactory Nerve
|Optic Nerve
|Oculomotor Nerve
|Trochlear Nerve
|Trigeminal Nerve
|Abducent Nerve
|Facial Nerve
|Vestibulocochlear Nerve
|Glossopharyngeal Nerve
|Vagus Nerve
|Accessory Nerve
|Hypoglossal Nerve
Trochlear Nerve (Cranial Nerve IV)
The trochlear nerve (CN IV) is the smallest cranial nerve and the only one to emerge dorsally from the brainstem. It innervates the superior oblique muscle, enabling downward and inward eye movement. Because it decussates within the midbrain, each nerve controls the contralateral eye.
🔎 Anatomy & Course
- Nucleus: Midbrain at level of inferior colliculus.
- Decussation: Fibres cross in the midbrain → each nerve supplies the opposite eye.
- Exit: Emerges dorsally, below inferior colliculus.
- Course: Wraps around cerebral peduncles → travels in subarachnoid space → runs beneath tentorium → cavernous sinus (lateral wall, below CN III) → enters orbit via superior orbital fissure (outside annulus of Zinn).
🧩 Innervation & Function
- Superior Oblique Muscle:
- Origin: sphenoid bone above tendinous ring.
- Trochlea: fibrocartilaginous pulley on medial orbital wall.
- Action: depression (in adduction), intorsion, assists in abduction.
⚡ Clinical Relevance
- Trochlear Nerve Palsy
- Causes: trauma (long intracranial course), diabetes/HTN, congenital, tumours/aneurysms, MS, raised ICP.
- Symptoms: vertical diplopia, worse on looking down & in (e.g. stairs, reading); head tilt away from lesion (Bielschowsky sign); hypertropia & extorsion.
- Diagnosis: clinical exam, Bielschowsky head-tilt test, MRI/CT if structural cause suspected.
- Treatment: prism glasses, strabismus surgery, treat underlying cause.
- Evaluation: Ask patient to follow “H” pattern; check for downward movement when adducted; observe for diplopia, misalignment, head posture.
📊 Differentials: CN IV vs III vs VI Palsy
| Nerve | Muscle(s) affected | Typical Findings |
|---|
| CN III (Oculomotor) | Most EOMs, levator, sphincter pupillae | “Down & out” eye, ptosis, dilated pupil |
| CN IV (Trochlear) | Superior oblique | Vertical diplopia, worse down/in; head tilt away from lesion |
| CN VI (Abducens) | Lateral rectus | Inability to abduct, horizontal diplopia |
📌 OSCE Exam Tips
- Always test eye movements in an “H” pattern – CN IV palsy shows deficit on downward gaze in adduction.
- Ask about difficulty with stairs/reading (classic complaint).
- Look for head tilt compensation away from the lesion side.
- Remember: CN IV lesions affect the contralateral superior oblique (because of decussation).
📚 References
- Standring S. Gray's Anatomy, 41st ed. Elsevier, 2016.
- Haines DE. Neuroanatomy, 9th ed. Wolters Kluwer, 2019.
- Jacobson DM. Ophthalmology. 2000;107(8):1504-1509.
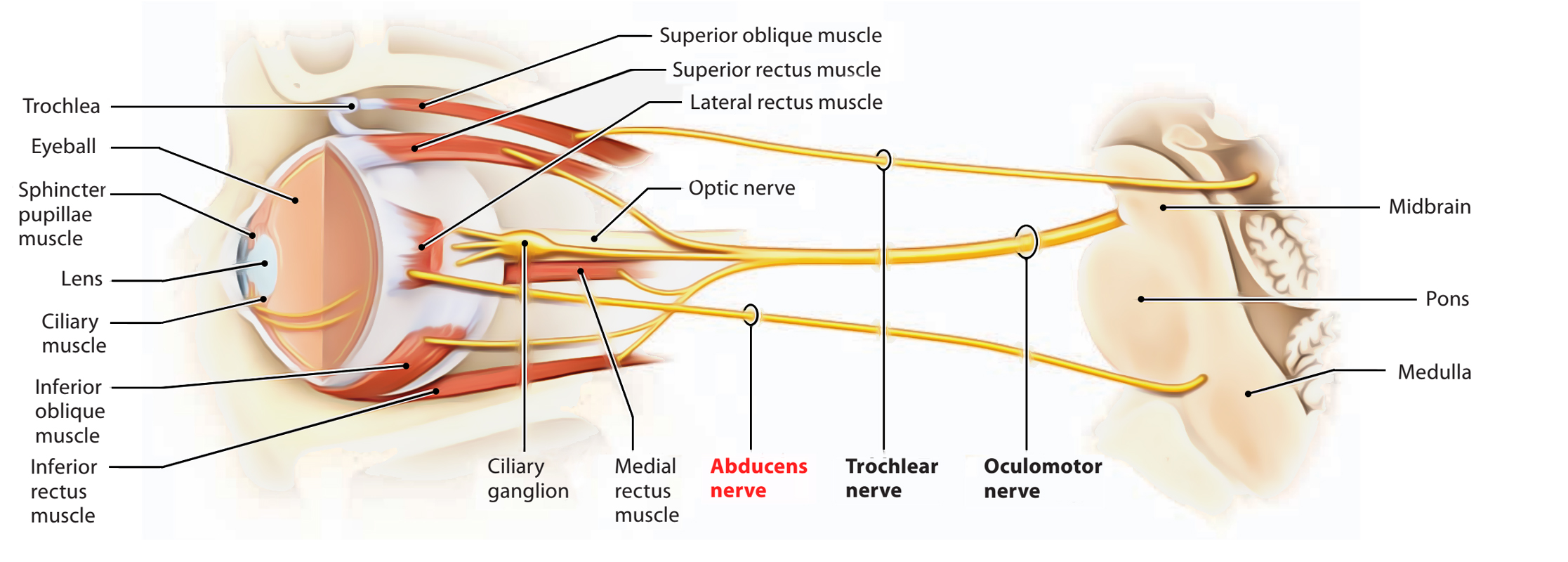
🖼️ Visuals
For diagrams of CN IV course and palsy features: