
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Body Mass Index
Related Subjects: |Malnutrition universal screening tool (MUST) |Body Mass Index |Peripherally inserted central catheters (PICC) |Refeeding syndrome
📖 Introduction
Body Mass Index (BMI) is a quick and widely used screening tool that relates an individual’s weight to their height, providing a numerical estimate of body fat. Although originally designed for population-level epidemiology by Adolphe Quetelet in the 19th century, it remains a key measure in modern clinical practice and public health. It is especially useful for flagging those at risk of undernutrition, overweight, or obesity, all of which carry significant health implications.
🧮 Calculation and Classification
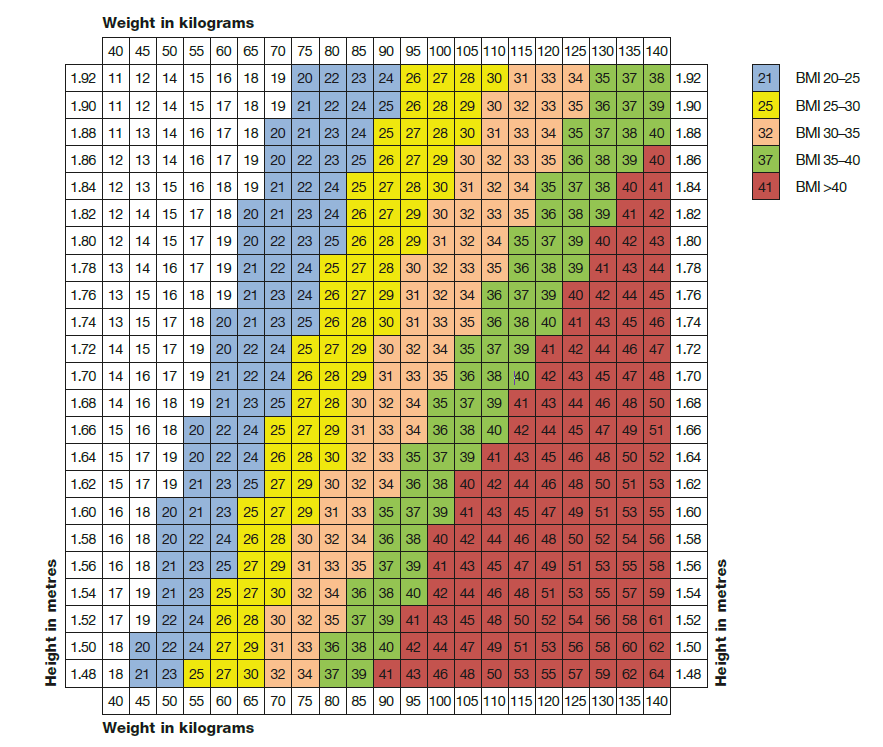
BMI is calculated using the standard formula:
BMI = Weight (kg) / [Height (m)]2
For adults, BMI is classified into categories (WHO/NICE):
- ⚠️ Underweight: <18.5
- ✅ Normal weight: 18.5 – 24.9
- ⚠️ Overweight: 25 – 29.9
- ⬆️ Obesity Class I: 30 – 34.9
- ⬆️ Obesity Class II: 35 – 39.9
- 🚨 Obesity Class III (Morbid obesity): ≥40
🏥 Clinical Significance
- 📊 Screening tool: Provides a rapid overview of nutritional status in both undernutrition and obesity.
- ❤️ Risk stratification: Higher BMI is associated with increased risk of type 2 diabetes, hypertension, cardiovascular disease, stroke, and some cancers.
- 🧩 Monitoring: Useful for following weight changes over time, particularly in patients on weight management programmes or nutritional support.
- 👶 Paediatrics: In children, BMI must be plotted against age- and sex-specific centile charts (UK-WHO growth charts) rather than adult cut-offs.
⚖️ Limitations of BMI
- 💪 Muscle vs fat: BMI does not distinguish lean mass from fat mass, so muscular individuals may appear “overweight.”
- 🧍 Fat distribution: Central obesity (visceral fat) carries more cardiometabolic risk than peripheral fat, but BMI alone cannot capture this.
- 🧓 Age & sex: Elderly patients may have sarcopenia (muscle loss) despite a “normal” BMI. Women generally have higher body fat at the same BMI than men.
- 🌍 Ethnic variation: In South Asian and Chinese populations, health risks occur at lower BMI thresholds → NICE advises using 23 kg/m² as the overweight threshold for these groups.
📌 Alternative / Complementary Measures
- Waist Circumference (WC): Better predictor of central obesity and metabolic syndrome risk. → Risk increased if WC >94 cm (men) or >80 cm (women).
- Waist-to-Height Ratio: >0.5 suggests increased cardiometabolic risk.
- Body Fat %: Measured by bioelectrical impedance or DEXA scanning, gives more accurate assessment of adiposity.
- Clinical context: Combine BMI with blood pressure, lipids, HbA1c, and lifestyle assessment.
🧭 Conclusion
BMI remains a simple, cost-effective, first-line screening tool for assessing nutritional status. However, it should never be used in isolation. Interpreting BMI alongside waist circumference, comorbidities, and demographic factors provides a more accurate picture of health risk. In UK practice, NICE and Public Health England recommend combining BMI with waist measures to guide interventions in obesity and metabolic risk.
📚 References
- NICE CG189: Obesity Identification, Assessment and Management
- WHO – Obesity and Overweight
- Public Health England. Adult Obesity: Applying All Our Health.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery