
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Adult Onset Stills Disease
Related Subjects: |Tennis Elbow |Golfer's Elbow |Painful Shoulder syndromes |Plantar fasciitis |Carpal tunnel syndrome |Chondrocalcinosis |Adult Onset Still's Disease
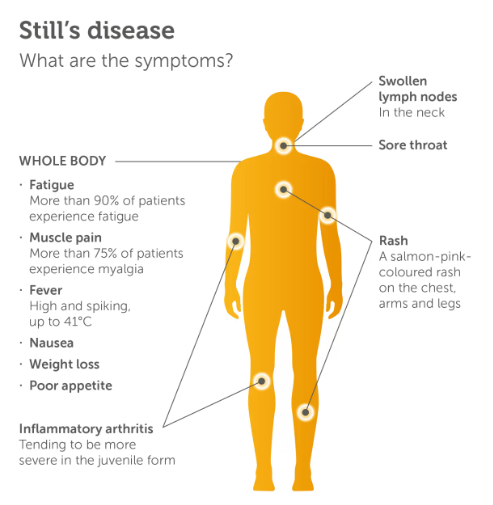
🔥 Adult-Onset Still's Disease (AOSD) is a rare systemic autoinflammatory disorder. It classically presents with high spiking fevers, arthralgia/arthritis, and a distinctive salmon-pink rash. Often mimics viral infection → consider in PUO cases with negative autoantibodies.
ℹ️ About
- Typically affects young adults (16–35 yrs).
- Often begins as pyrexia of unknown origin (PUO).
- Suspected viral trigger in some cases.
👩⚕️ Clinical Features
- Daily spiking fevers up to 40°C 🌡️ with sweats & chills.
- Severe sore throat (common early feature).
- Rash: salmon-pink, evanescent, maculopapular (often on trunk & proximal limbs, worse with fever spikes).
- Weight loss, malaise, hepatosplenomegaly, lymphadenopathy.
- Arthralgia → chronic destructive arthritis in late disease.
🔬 Investigations
- RF and ANA negative (helps exclude RA & lupus).
- ↑ ESR, ↑ CRP.
- Leukocytosis (WCC often >40,000) with neutrophilia.
- Thrombocytosis.
- Ferritin markedly raised (>3000 ng/mL is highly suggestive).
⚠️ Complication: Macrophage Activation Syndrome (MAS)
- Life-threatening “cytokine storm” syndrome with pancytopenia, DIC, liver failure.
- Triggered by excessive immune activation.
- Treatment: High-dose corticosteroids ± immunosuppressants (e.g. ciclosporin, biologics).
💊 Management
- 🟢 Mild disease: NSAIDs (e.g. aspirin 1 g TDS, ibuprofen).
- 🟠 Moderate/severe: Corticosteroids (e.g. prednisolone 40–60 mg/day).
- ⚙️ Disease-modifying therapy: Methotrexate for steroid-sparing effect.
- 🧬 Biologics:
- TNF inhibitors (etanercept, infliximab).
- IL-1 inhibitors (anakinra, canakinumab).
- IL-6 inhibitors (tocilizumab).
Cases - Adult-Onset Still’s Disease (AOSD)
- Case 1 - Classic triad 🔥: A 28-year-old woman presents with daily spiking fevers for 2 weeks, evanescent salmon-pink macular rash on trunk/arms, and polyarthritis affecting wrists and knees. Bloods: markedly raised ferritin (>5000 µg/L), neutrophilia, raised CRP/ESR. ANA and RF negative. Diagnosis: classic AOSD. Managed with NSAIDs and corticosteroids.
- Case 2 - Systemic features 🫁: A 35-year-old man presents with fever, sore throat, lymphadenopathy, hepatosplenomegaly, and pleuritic chest pain. Labs: ferritin 10,000 µg/L, abnormal LFTs, leukocytosis. Excluded infection and lymphoma. Diagnosis: systemic AOSD with serositis. Treated with steroids; later escalated to methotrexate for steroid-sparing effect.
- Case 3 - Severe complication 🫀: A 41-year-old woman with known AOSD is admitted with shock, fever, cytopenias, coagulopathy, and high ferritin. Diagnosed with macrophage activation syndrome (MAS), a life-threatening complication of Still’s disease. Managed in ITU with IV methylprednisolone and ciclosporin, with haematology input.
Teaching Point 🩺: Adult-onset Still’s disease is an autoinflammatory disorder characterised by quotidian fevers, evanescent rash, and arthritis. Ferritin is often massively elevated. Always rule out infection, malignancy, and autoimmune mimics. MAS/HLH is a feared complication.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery