
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Juvenile Idiopathic Arthritis (Stills Disease)
Related Subjects: | Monoarticular Arthritis | Polyarticular Arthritis | Seronegative Spondyloarthropathies | Ankylosing Spondylitis | Enteropathic Spondyloarthritis | Reactive Arthritis | Psoriatic Arthritis
🧒 Juvenile Idiopathic Arthritis (JIA) is the most common chronic rheumatic disease of childhood. Aspirin should be avoided in children <12 due to the risk of Reye’s syndrome ⚠️. Tumour necrosis factor (TNF) 🧬 is a key pro-inflammatory cytokine in JIA pathogenesis.
📖 About
- Accounts for ~10% of all chronic arthritis in children.
- Onset usually <16 years (often <5 years).
- Systemic form may mimic infection or malignancy.
- Adult-onset Still’s disease is the adult equivalent, but rare.
🧬 Aetiology
- Equal male:female in systemic type; other subtypes more female.
- Genetic predisposition – HLA associations.
- Environmental triggers (infections, stress, trauma) may unmask disease.
- Pathogenesis: imbalance of Th1 (IFN-γ) and Th17 (IL-17) cells + dysregulated innate immunity (IL-1, IL-6, TNF-α).
🔑 Definitions
- Oligoarthritis: ≤4 joints in first 6 months.
- Polyarthritis: ≥5 joints in first 6 months.
- Systemic JIA (sJIA): Autoinflammatory form with fever + rash + organ involvement.
🌈 Subtypes
- Oligoarthritis – 50–60%.
- RF+ polyarthritis – 11–28% (resembles adult RA).
- RF– polyarthritis – 2–7%.
- Systemic JIA: 🩸 High spiking fevers, salmon-pink rash, lymphadenopathy, hepatosplenomegaly, serositis.
- Psoriatic arthritis 🎨.
- Enthesitis-related arthritis 🦶 – HLA-B27 associated.
- Undifferentiated arthritis.
🤒 Classic Clinical Features (Systemic JIA)
- Daily high fevers (>39°C), often evening spikes 🌡️.
- Transient pink/salmon maculopapular rash 🌸.
- Arthralgia/arthritis (sometimes late feature).
- Other: lymphadenopathy, hepatosplenomegaly, myocarditis, pericarditis, pleurisy, dry eyes (uveitis risk).
- ~50% risk of chronic destructive arthritis long-term 🦴.
🔎 Investigations
- Bloods: ↑ ESR, ↑ CRP, ↑ ferritin 📈 (esp. systemic JIA).
- FBC: Anaemia of chronic disease, ↑ neutrophils, ↑ platelets.
- Autoantibodies usually negative (ANA, RF, HLA-B27). ⚠️ High RF or ANA positivity may point to alternative diagnoses.
- Imaging: – X-rays may be normal early. – 🖥️ Ultrasound: synovial thickening, effusion, tenosynovitis. – MRI: 🥇 gold standard – detects bone marrow oedema and erosions.
🩺 Differentials
- Oligoarthritis mimics: Reactive arthritis, toxic synovitis, septic arthritis, osteomyelitis, haemophilia, sickle cell, trauma/NAT, tumours.
- Polyarthritis mimics: SLE, MCTD, rheumatic fever, IBD-related arthritis, sarcoid, CRMO.
- Systemic mimics: Infections (mycoplasma, EBV, endocarditis), Kawasaki disease, PFAPA, malignancy (ALL, lymphoma), autoinflammatory syndromes.
⚠️ Complications
- Growth disturbance & leg-length discrepancy.
- Joint contractures & disability.
- Macrophage activation syndrome (MAS) – life-threatening cytokine storm 🛑.
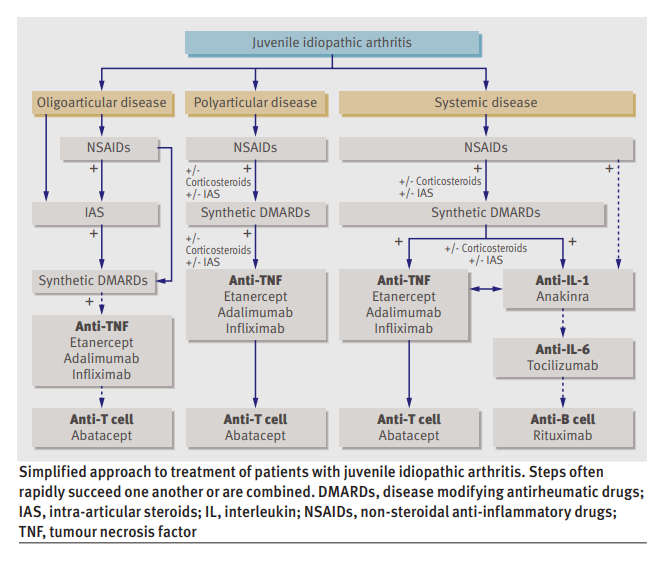
💊 Management
- All suspected JIA → urgent referral to paediatric rheumatology 👩⚕️.
- NSAIDs for pain & stiffness (avoid aspirin in <12).
- Steroids (systemic or intra-articular) for acute flares or organ involvement.
- Methotrexate – cornerstone steroid-sparing agent.
- Biologics: Anti-TNF (etanercept, adalimumab), IL-1 (anakinra), IL-6 (tocilizumab) for refractory cases 🧬.
- Vaccination: Avoid live vaccines if immunosuppressed. Annual flu 💉 recommended.
- Monitor growth, eye health (uveitis risk), and bone health (steroids + inactivity risk).
📚 References
Case – Systemic Juvenile Idiopathic Arthritis (Still’s disease)
A 9-year-old presents with 2 weeks of daily quotidian fevers peaking late afternoon, an evanescent salmon-pink rash appearing with fever, migratory arthralgia now localising to both knees, and sore throat; exam shows hepatosplenomegaly and mild lymphadenopathy. Labs: markedly ↑CRP/ESR, neutrophilia, anaemia, thrombocytosis, and very high ferritin (low glycosylated fraction if tested); cultures negative; CXR normal. After excluding infection and malignancy, diagnose systemic JIA; screen vigilantly for macrophage activation syndrome (MAS) (cytopenias, rising ferritin with falling ESR, ↑ALT, ↑triglycerides). Management: start systemic glucocorticoids for control and escalate early to targeted therapy-IL-1 blockade (anakinra) or IL-6 blockade (tocilizumab)-with physiotherapy and bone/gastroprotection; involve paediatric rheumatology and monitor joints, growth, LFTs, and MAS red flags.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery