
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Graves Disease (Thyrotoxicosis) ✅
Related Subjects: |Thyrotoxicosis and Hyperthyroidism |Thyroid Storm - Thyrotoxic crisis |Graves' Disease (Thyrotoxicosis) |Amiodarone and Thyroid disease |Thyroid Surgery (Thyroidectomy) |Hypothyroidism |Hashimoto's thyroiditis |DeQuervain's thyroiditis |Subacute Thyroiditis |Thyroid nodule |Congenital Hypothyroidism |Thyroid Function Tests and antibodies |Post partum thyroiditis |Sick Euthyroid Syndrome |Thyroid Exam (OSCE) |Thyroid Gland anatomy and Physiology |Thyroid Cancer
⚠️ Smokers with Graves' Disease have a significantly higher risk of developing thyroid eye disease (TED). Smoking cessation is essential to reduce complications and improve outcomes. 💨
📖 About
- Autoimmune disease: Graves’ disease is the most common cause of hyperthyroidism (60–80% of cases).
- Leading cause of thyrotoxicosis in the UK and worldwide.
- Immune-mediated stimulation of TSH receptors drives thyroid hormone overproduction.
🔎 Risk Factors
- Gender: Women >> Men (~10:1).
- Age: Typically 30–50 years.
- Postpartum: Increased risk in first 6–12 months.
- Smoking: Major modifiable risk factor for TED; worsens severity and prognosis.
- Family history: Genetic predisposition via HLA-B8, DR3.
🧬 Pathophysiology & Aetiology
- TSH receptor antibodies (TRAb): Stimulate follicular hyperplasia, ↑ T3/T4 production; cross placenta → neonatal thyrotoxicosis.
- Thyroid peroxidase antibodies (TPOAb): Present in ~80%.
- Orbital fibroblast activation: Glycosaminoglycan deposition → proptosis, diplopia, orbital oedema.
- Autoimmunity can be triggered by infections, stress, or iodine exposure.
🩺 Clinical Presentation
- Symptoms: Weight loss, heat intolerance, palpitations, anxiety, tremor, diarrhoea.
- Elderly: May present with apathetic thyrotoxicosis – fatigue, anorexia, atrial fibrillation.
- Examination: Diffuse, smooth goitre with bruit/thrill, tremor, warm moist skin, tachycardia, hyperreflexia.
🌟 Specific Signs
- Thyroid Eye Disease (TED): Lid lag, lid retraction, proptosis, diplopia, corneal ulceration (~40% of patients).
- Pretibial myxoedema: Non-pitting, pink-orange plaques (~5%).
- Thyroid acropachy: Rare clubbing with onycholysis.
🔬 Investigations (NICE & ATA Guidelines)
- Thyroid function tests: ↑Free T4/T3, suppressed TSH (<0.05 mIU/L).
- TRAb: Confirms autoimmune aetiology; predicts risk of TED.
- Radionuclide uptake scan: Diffuse uptake in Graves’, distinguishes from toxic adenoma/multinodular goitre.
- Thyroid ultrasound: Optional; evaluates nodularity.
- Ophthalmology assessment: Baseline visual acuity, colour vision, intraocular pressure, exophthalmometry for TED severity.
🧾 Differentials
- Toxic multinodular goitre
- Toxic adenoma
- Exogenous thyroxine excess
- Subacute thyroiditis (painful, self-limiting)
⚕️ Management (NICE & ATA/ETA Guidance)
- Symptom control: Beta-blockers (propranolol 20–40 mg QDS) for palpitations, tremor, anxiety.
- Antithyroid drugs (ATDs): Carbimazole first-line (20–40 mg daily titrated), propylthiouracil reserved for pregnancy or intolerance.
- Radioiodine therapy: Avoid in active TED, particularly smokers; may worsen ophthalmopathy.
- Surgery: Subtotal or total thyroidectomy for severe, compressive, or refractory disease.
- Atrial fibrillation: Consider anticoagulation per CHA₂DS₂-VASc; monitor for hyperthyroid-related cardiomyopathy.
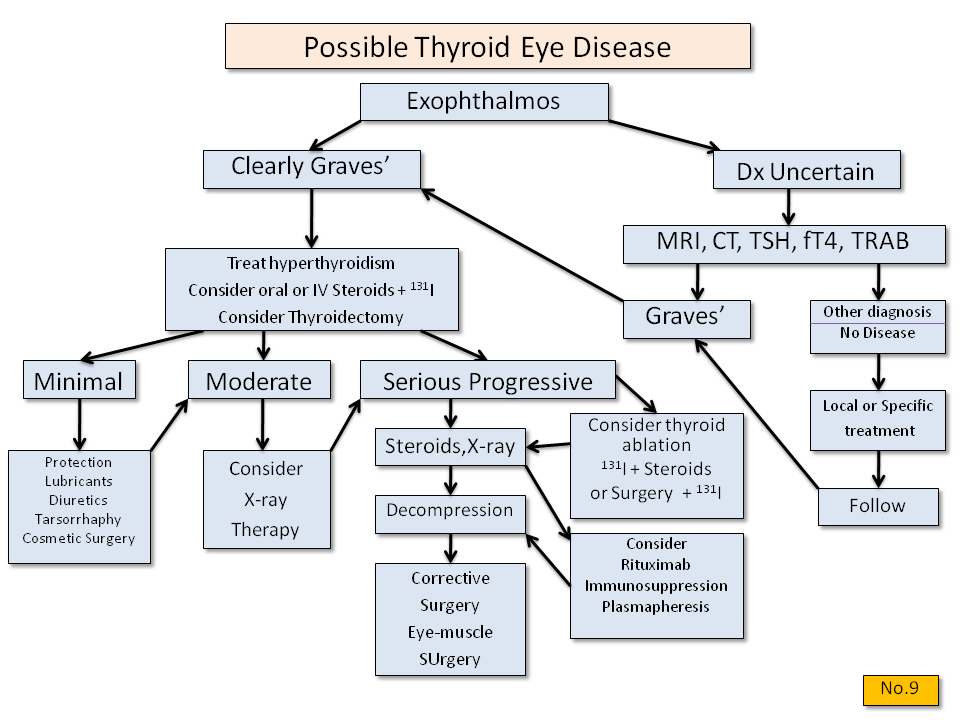
👁️ Thyroid Eye Disease (TED) Management
- Initial muscle involved: Inferior rectus → restricted upgaze.
- Smoking cessation: Most important modifiable factor.
- Ophthalmology referral: Monitor acuity, optic nerve function, intraocular pressure.
- Conservative: Lubricants, eyelid taping, head elevation, selenium supplementation if mild.
- Medical therapy: IV/oral glucocorticoids (prednisolone 60 mg), immunomodulators (ciclosporin, rituximab, teprotumumab where available).
- Advanced: Orbital radiotherapy or surgical decompression in sight-threatening disease.
💡 Exam Tips
• Hyperthyroid patient who smokes → always ask about eye symptoms; early TED referral improves prognosis.
• TRAb positive → confirms Graves’ and risk stratification for TED.
• Active TED = contraindication to radioiodine therapy.
• Diffuse goitre with bruit → hallmark on palpation.
• Pretibial myxoedema or acropachy → pathognomonic but rare.
📚 References
- NICE NG145: Thyroid disease – assessment and management
- ATA Guidelines: 2016 Hyperthyroidism Management
- ETA/Endocrine Society: Thyroid Eye Disease Guidelines
- Ross DS, et al. 2016. American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis. Thyroid. 26(10):1343–1421.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery