
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Hypocalcaemia ✅
Related Subjects: |Calcium Physiology |Calcitonin |Hypocalcaemia |Hypercalcaemia |Hypomagnesaemia |Hypermagnesaemia |Primary Hyperparathyroidism |Familial hypocalciuric hypercalcaemia (FHH) |Sarcoidosis
⚠️ Always check magnesium in hypocalcaemia. Hypomagnesaemia can both reduce PTH secretion and cause end-organ resistance to PTH, making hypocalcaemia refractory until Mg²⁺ is corrected.
| 🚨 Acute / Severe Hypocalcaemia: Initial Management
Always ask: Is the patient symptomatic? Are they on digoxin? Is magnesium low? |
|---|
|
🔢 Corrected / Adjusted Calcium Ranges
| Category | Adjusted Ca (mmol/L) |
|---|---|
| ✅ Normal | About 2.20–2.60 |
| ⬇️ Mild hypocalcaemia | 1.90–2.19 and asymptomatic |
| 🚨 Severe hypocalcaemia | <1.90 or symptomatic at any level below normal |
📌 Use adjusted calcium for routine interpretation, but consider ionised calcium in critical illness, major acid–base disturbance, or when albumin makes total calcium misleading.
🧬 Aetiology & Pathophysiology
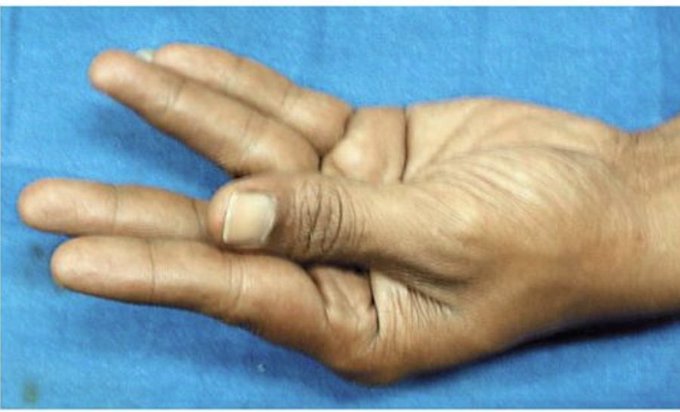
- ⚡ Low extracellular Ca²⁺ lowers the threshold for membrane depolarisation, causing neuromuscular hyperexcitability → paraesthesia, tetany, carpopedal spasm, laryngospasm, and seizures.
- ❤️ Cardiac repolarisation is prolonged, producing a long QT interval and increasing arrhythmia risk.
- 🧂 Mg²⁺ deficiency is important because it can cause both impaired PTH release and PTH resistance.
📊 Common Causes of Hypocalcaemia
| Cause | Typical Clues | Biochemistry Pattern | Management Principles |
|---|---|---|---|
| Hypoparathyroidism
(post-thyroid/parathyroid surgery, autoimmune, infiltrative) |
Perioral tingling, tetany, post-op neck surgery | Low Ca, low or inappropriately normal PTH, often high phosphate | Calcium ± alfacalcidol/calcitriol; treat acute episodes with IV calcium if severe |
| Vitamin D deficiency | Bone pain, proximal myopathy, osteomalacia/rickets risk | Low/low-normal Ca, low vitamin D, raised PTH, often low phosphate | Vitamin D replacement ± calcium |
| CKD / reduced 1α-hydroxylation | Renal disease, CKD-MBD features | Low Ca, high phosphate, raised PTH, reduced active vitamin D | Manage CKD-MBD, phosphate control, active vitamin D analogues, calcium as needed |
| Hypomagnesaemia | Alcohol excess, diarrhoea, PPIs, diuretics, aminoglycosides | Low Mg, low Ca, PTH low or inappropriately normal | Replace Mg first / alongside Ca |
| Acute pancreatitis | Severe epigastric pain, vomiting | Low Ca, raised amylase/lipase | Supportive pancreatitis care; calcium if severe/symptomatic |
| Pseudohypoparathyroidism | Possible Albright hereditary osteodystrophy phenotype | Low Ca, high PTH, high phosphate | Calcium + active vitamin D; endocrine follow-up |
| Drugs
(bisphosphonates, denosumab, cisplatin, foscarnet, anticonvulsants, cinacalcet) |
Temporal relationship to treatment | Variable, depending on mechanism | Stop/review culprit drug, replace calcium ± Mg/vitamin D |
| Sepsis / critical illness | Shock, organ dysfunction | Low Ca in context of severe illness | Treat underlying illness; reserve IV calcium for severe/symptomatic cases |
| Hungry bone syndrome | After parathyroid surgery, high bone turnover states | Marked/prolonged low Ca ± low Mg ± low phosphate | Aggressive calcium replacement + active vitamin D |
| Massive transfusion / citrate load | Major haemorrhage / blood product exposure | Low ionised calcium | Correct as part of major haemorrhage management |
⚡ Clinical Features
- Acute: Perioral/fingertip paraesthesia, muscle cramps, carpopedal spasm, tetany, positive Trousseau’s/Chvostek’s sign, laryngospasm/stridor, seizures, prolonged QT.
- Chronic: Cataracts, dry skin, brittle nails, poor dentition, basal ganglia calcification, neuropsychiatric symptoms.
🧪 Investigations
- First-line bloods: adjusted calcium, albumin, Mg²⁺, phosphate, U&E/creatinine, PTH, 25-OH vitamin D.
- Consider ionised calcium if critically ill or the total/adjusted calcium may be unreliable.
- ECG: prolonged QT ± arrhythmia.
- Think about cause: recent thyroid/parathyroid surgery, CKD, pancreatitis, malabsorption, alcohol excess, blood transfusion, denosumab/bisphosphonate use, PPIs.
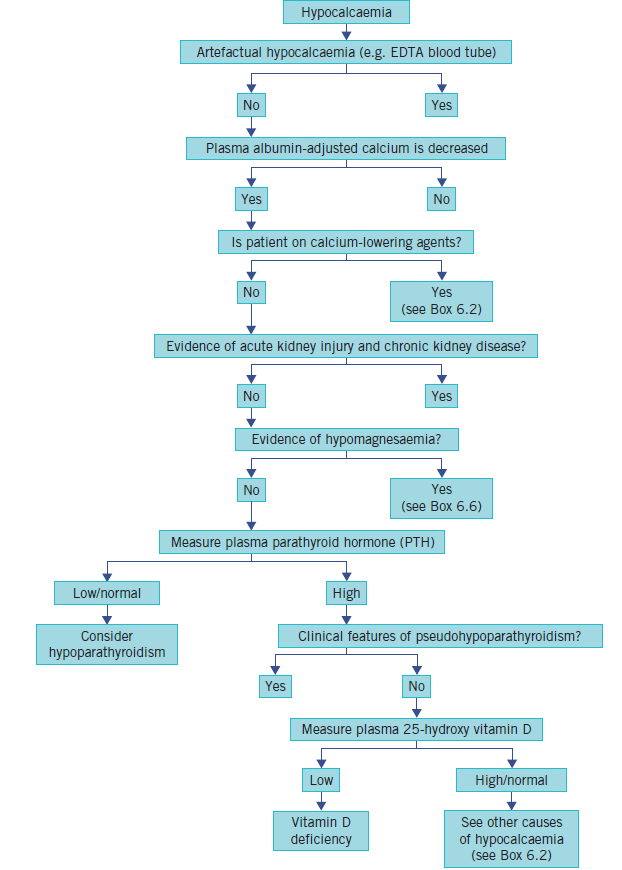
📈 Interpretation Patterns
- Low Ca + low / inappropriately normal PTH → hypoparathyroidism or severe hypomagnesaemia.
- Low Ca + high PTH → vitamin D deficiency, CKD, pseudohypoparathyroidism, pancreatitis, sepsis, or other secondary causes.
- Low Ca + low Mg → correct Mg early, as calcium may remain refractory otherwise.
- Low Ca + high phosphate → think hypoparathyroidism, CKD, or pseudohypoparathyroidism.
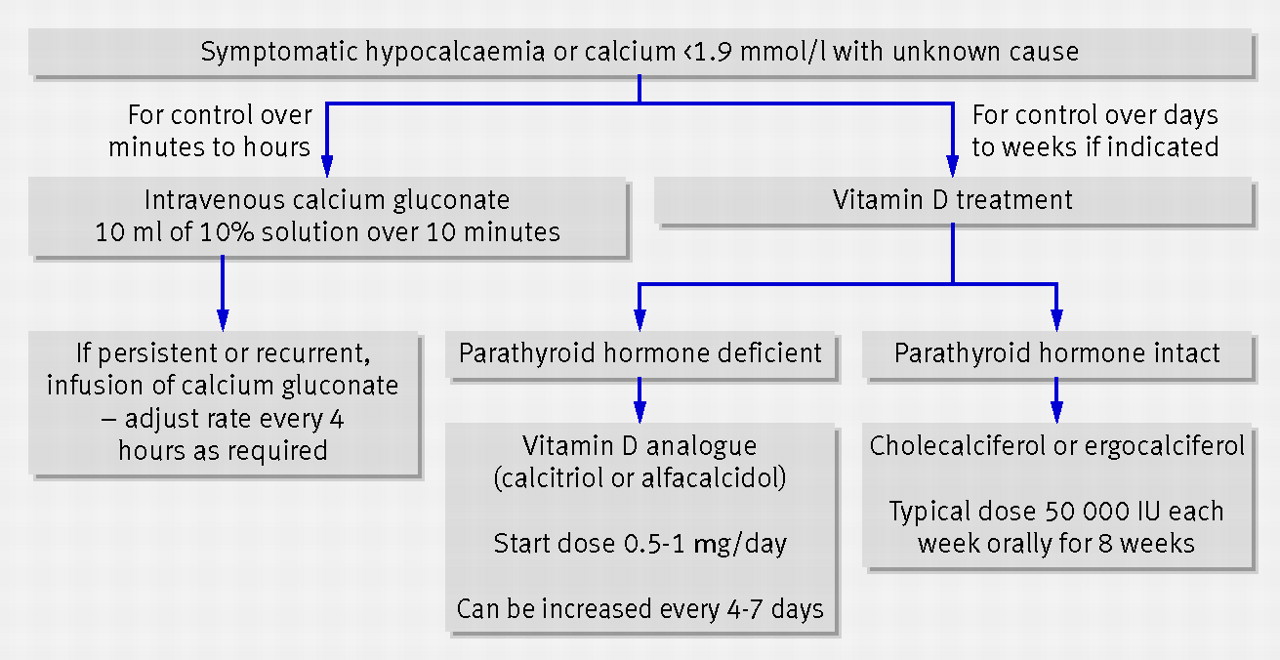
💊 Practical Management Summary
- Mild, asymptomatic hypocalcaemia (1.9–2.19 mmol/L): oral calcium, investigate cause, recheck calcium after correction begins.
- Severe or symptomatic hypocalcaemia: IV calcium gluconate with monitoring, then infusion if needed.
- Correct magnesium and address the underlying pathology.
- Use active vitamin D when hypoparathyroidism or impaired renal activation is likely.
- Avoid rapid IV administration because it can cause flushing, nausea, hypotension, and arrhythmias.
📚 References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery