Related Subjects:
|ECG Basics
|ECG Axis
|ECG Analysis
|ECG LAD
|ECG RAD
|ECG Low voltage
|ECG Pathological Q waves
|ECG ST/T wave changes
|ECG LBBB
|ECG RBBB
|ECG short PR
|ECG Heart Block
|ECG Asystole and P wave asystole
|ECG QRS complex
|ECG ST segment
|ECG: QT interval
|ECG: LVH
|ECG RVH
|ECG: Bundle branch blocks
|ECG Dominant R wave in V1
|ECG Acute Coronary Syndrome
|ECG Crib sheets
🧠 In all cases: look for the cause and clinical context
- 🔍 Always look for reversible causes such as:
- ischaemia / acute myocardial infarction
- drug effects (for example beta-blockers, digoxin, verapamil, diltiazem, amiodarone)
- electrolyte disturbance, especially hyperkalaemia
- hypothyroidism
- infection, hypothermia, raised vagal tone, or post-cardiac procedure conduction injury
- 💊 If drugs are contributing and the patient is symptomatic, reduce or stop them where appropriate.
- 🚑 If bradycardia is causing compromise, give atropine 500 micrograms IV; repeat if needed to a maximum of 3 mg.
- ⚠️ If there are life-threatening features or a high risk of asystole, seek urgent senior help and prepare for pacing and/or vasoactive support.
- 🔌 A pacemaker is the definitive treatment for many persistent or high-risk bradyarrhythmias, especially when the block is not readily reversible.
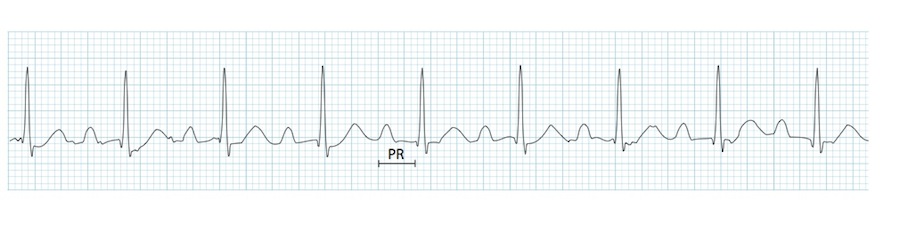
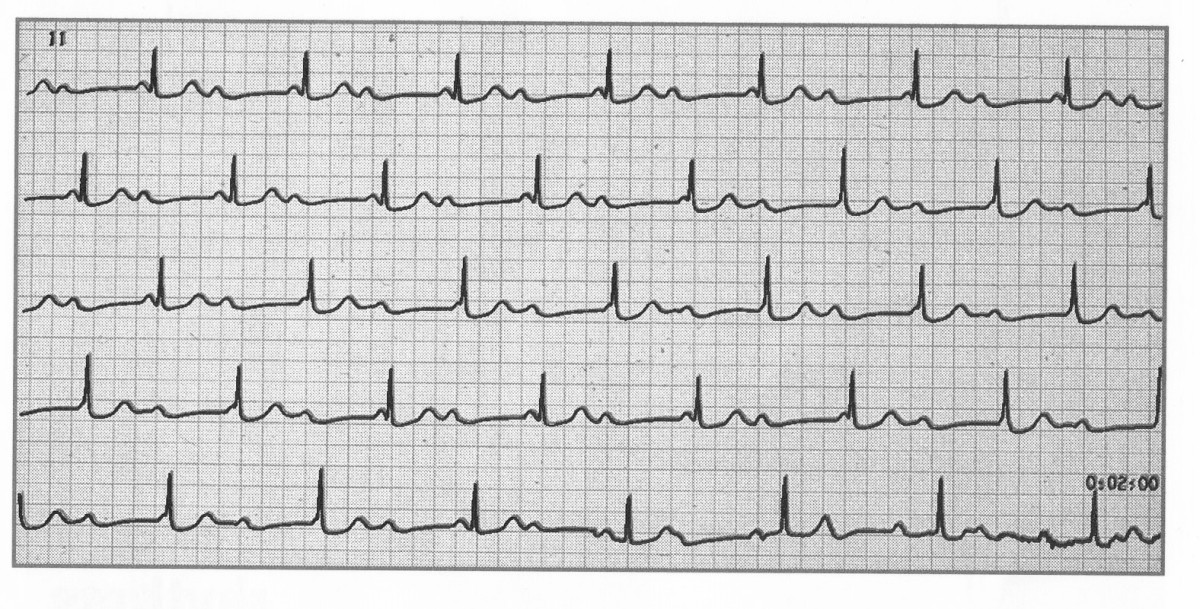
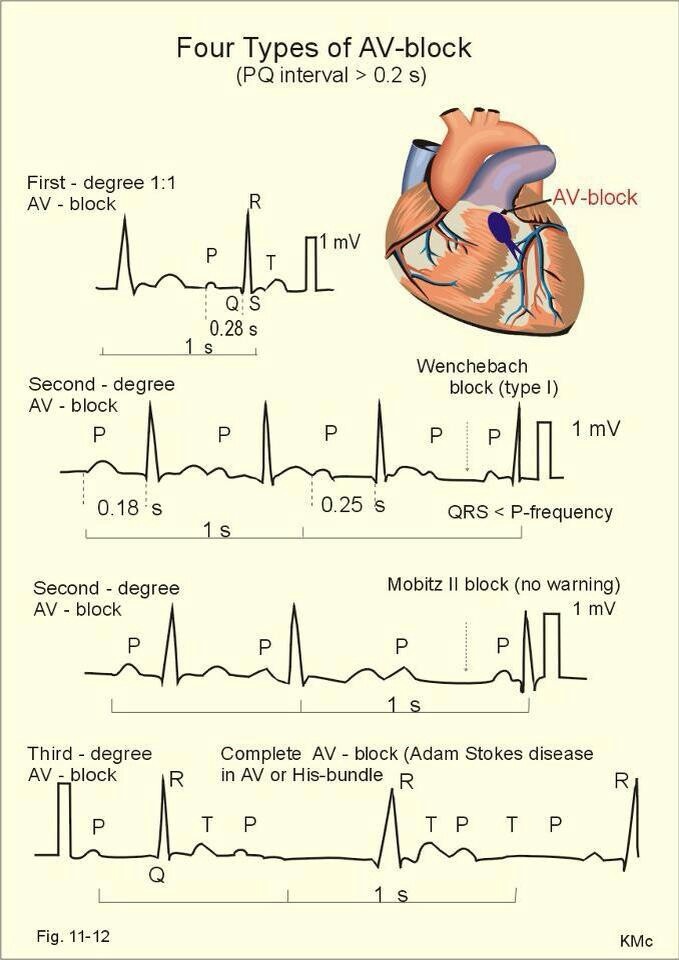
🟢 First-degree AV block
- Definition: delayed AV conduction with a PR interval > 0.20 seconds, but every P wave is still followed by a QRS complex.
- Rate: can occur with either sinus bradycardia or sinus tachycardia.
- Rhythm: sinus rhythm, regular.
- PR interval: prolonged and fixed.
- P waves: normal morphology; every P wave is followed by a QRS, and every QRS is preceded by a P wave.
- QRS: usually narrow unless there is additional intraventricular conduction disease.
- 😊 Usually not clinically significant and often requires no specific treatment.
- ⚠️ Important exception: progressive PR prolongation in infective endocarditis can suggest an aortic root abscess.
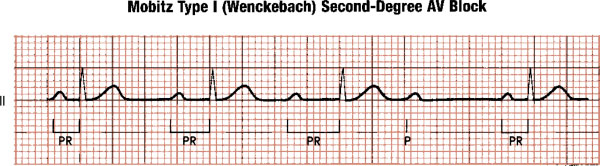
🟡 Mobitz type I (Wenckebach)
- Definition: progressive prolongation of the PR interval until a P wave is not followed by a QRS complex.
- Atrial rhythm: regular.
- Ventricular rhythm: irregular because of the dropped beats.
- PR interval: lengthens progressively from beat to beat, then one beat is dropped.
- P waves: normal in shape; occasional P wave not conducted.
- QRS: usually narrow, suggesting nodal-level block.
- 📍 This is often an AV nodal block and can be seen in healthy people, athletes, or with high vagal tone.
- 😊 It often does not require pacing unless it causes significant symptoms or occurs in a concerning clinical context.

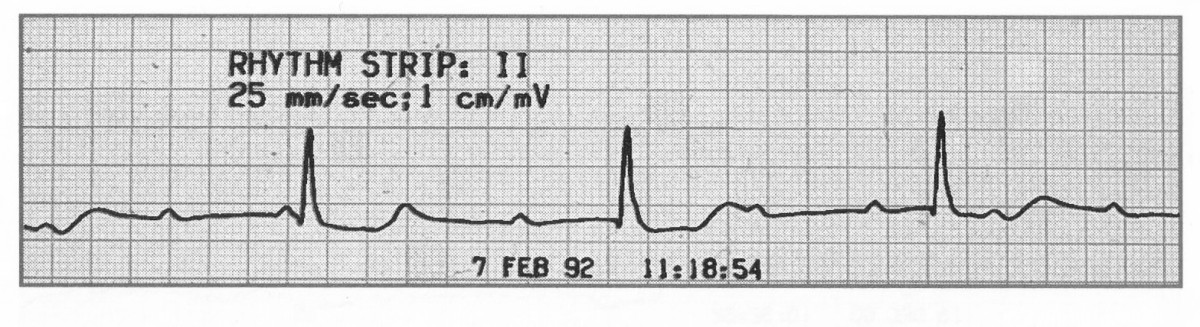
🟠 Mobitz type II
- Definition: intermittent non-conducted P waves without progressive PR prolongation.
- Atrial rate: usually regular.
- Ventricular rate: slower than the atrial rate because some impulses are blocked.
- Rhythm: atrial rhythm regular; ventricular rhythm may be irregular because of dropped beats.
- PR interval: constant in conducted beats.
- P waves: normal morphology, but some are not followed by QRS complexes.
- QRS: may be narrow or wide; a wide QRS suggests more distal conduction system disease and higher risk.
- ⚠️ More serious than Mobitz I because it can progress to complete heart block or asystole.
- 🔌 Management usually involves urgent specialist review and often pacing, unless there is a clearly reversible cause.
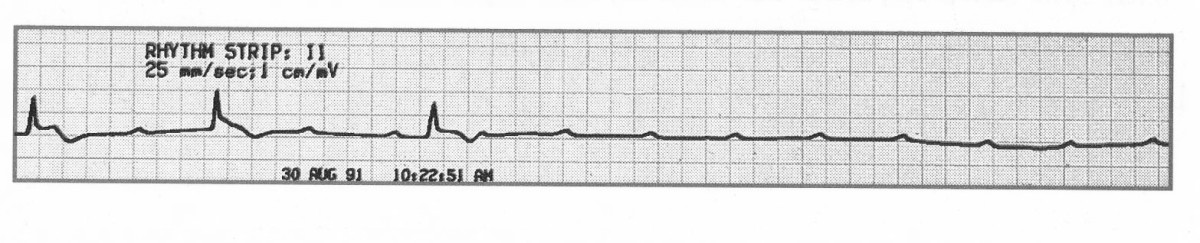
🔴 Third-degree (complete) heart block
- Definition: complete failure of AV conduction, so the atria and ventricles beat independently (AV dissociation).
- Atrial rate: usually determined by the sinus node and often 60–100 bpm.
- Ventricular rate: maintained by an escape rhythm and is usually slower.
- Rhythm: atrial rhythm and ventricular rhythm are both regular, but there is no relationship between them.
- PR interval: variable, because P waves and QRS complexes are dissociated.
- P waves: normal and regular.
- QRS: narrow if the escape rhythm is junctional; broad if ventricular, which is generally more unstable.
- 🚨 This may occur acutely, for example after myocardial infarction, and can sometimes be reversible depending on the cause and site of block.
- ⚠️ In symptomatic patients, this is a medical emergency and usually requires temporary pacing followed by assessment for a permanent pacemaker if the cause is not reversible.
💡 Practical clinical pearls
- 🩺 Not all AV block needs pacing, but Mobitz II and complete heart block should always be taken seriously.
- 📉 A broad-QRS complete heart block is especially high risk because it implies more distal conduction system disease.
- 💉 Atropine may help nodal bradycardia, but is often less effective in distal infranodal block.
- 🔍 Always ask: Is there a reversible cause?
- 🚑 If the patient is shocked, syncopal, ischaemic, or in heart failure, escalate early for pacing support.
